You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EmployeeHandbook PDFDocument50 pagesEmployeeHandbook PDFdhey Gonzales89% (9)
- Loan and Mortgage Agreement: For End-User Home Financing ProgramDocument7 pagesLoan and Mortgage Agreement: For End-User Home Financing ProgramPermits & LicensingNo ratings yet
- MLI Waiver IEPDocument1 pageMLI Waiver IEPArena NatubaNo ratings yet
- Mercantile LawDocument7 pagesMercantile LawAliNo ratings yet
- This Study Resource Was: Income Taxation (Final Exam) Multiple ChoiceDocument6 pagesThis Study Resource Was: Income Taxation (Final Exam) Multiple ChoiceGirly CrisostomoNo ratings yet
- Letter To State Agencies Requesting Budget CutsDocument2 pagesLetter To State Agencies Requesting Budget CutscallertimesNo ratings yet
- Business Finance (WEEK - 2-3)Document10 pagesBusiness Finance (WEEK - 2-3)Mizuki YamizakiNo ratings yet
- Module 11 PWCS Student WorkbookDocument6 pagesModule 11 PWCS Student WorkbookCricket DavisNo ratings yet
- Takaful Course & OutlineDocument2 pagesTakaful Course & OutlineAnonymous HlEh2INo ratings yet
- Geriatric Considerations in NursingDocument8 pagesGeriatric Considerations in NursingSathish Rajamani100% (6)
- 3001 A 184552264 00 B00 PyDocument2 pages3001 A 184552264 00 B00 PyRaghu DsNo ratings yet
- Introduction To Health Economics: Dr. Katie Sauer University of Southern Indiana Kmsauer1@usi - EduDocument26 pagesIntroduction To Health Economics: Dr. Katie Sauer University of Southern Indiana Kmsauer1@usi - EduKatherine SauerNo ratings yet
- Basics of Accounting - 4-5-21Document2 pagesBasics of Accounting - 4-5-21Mrutyunjay SaramandalNo ratings yet
- State Life Insurance Corporation of PakistanDocument39 pagesState Life Insurance Corporation of PakistanAsad Mazhar50% (4)
- Form of Business Ownership: General Partnership Limited PartnershipDocument7 pagesForm of Business Ownership: General Partnership Limited PartnershipJessabel Rosas BersabaNo ratings yet
- Appointment Reciept DURGA PRASADDocument3 pagesAppointment Reciept DURGA PRASADakash agarwalNo ratings yet
- Fitness Program: Save On Health Club Memberships, Exercise Equipment and More!Document1 pageFitness Program: Save On Health Club Memberships, Exercise Equipment and More!KALAI TIFYNo ratings yet
- Gsis Vs PalmieryDocument4 pagesGsis Vs Palmieryjoyce magtibayNo ratings yet
- LIABILITIESDocument12 pagesLIABILITIESJOHANNANo ratings yet
- Chapter 01 InsuranceDocument17 pagesChapter 01 InsuranceMd Rabbi KhanNo ratings yet
- SBI - Life - Smart - Wealth - Assure - V03 - Brochure - 20 - 1Document15 pagesSBI - Life - Smart - Wealth - Assure - V03 - Brochure - 20 - 1sunder vermaNo ratings yet
- The Early History of Insurance LawDocument18 pagesThe Early History of Insurance LawPamela Denise RufilaNo ratings yet
- Tinkoff Lifestyle Banking StrategyDocument46 pagesTinkoff Lifestyle Banking StrategyLinh Phuong Nguyen PhamNo ratings yet
- Booking 09.22.23 4142946Document1 pageBooking 09.22.23 4142946Superfresh OlvidameNo ratings yet
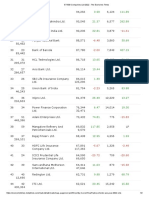
- 26-50 ET 500 Company List 2022Document2 pages26-50 ET 500 Company List 20220000000000000000No ratings yet
- MR - Ramesh Rao DDocument3 pagesMR - Ramesh Rao DrameshraodNo ratings yet
- Taxation of Residual Income: Cma K.R. RamprakashDocument25 pagesTaxation of Residual Income: Cma K.R. RamprakashShriya JoseincheckalNo ratings yet
- Access Florida Application Details 657074801Document5 pagesAccess Florida Application Details 657074801Norman AndrewsNo ratings yet
- Inmt 3Document31 pagesInmt 3shriyans varmaNo ratings yet
- Innovation Unlocks Access Transforming Healthcare Towards UHCDocument2 pagesInnovation Unlocks Access Transforming Healthcare Towards UHCkvn quintosNo ratings yet