You might also like
- Integrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionFrom EverandIntegrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionNo ratings yet
- Damodaram Sanjivayya National Law University, Nyayaprastha, Sabbavaram, Visakhapatnam, Andhra Pradesh-531035Document20 pagesDamodaram Sanjivayya National Law University, Nyayaprastha, Sabbavaram, Visakhapatnam, Andhra Pradesh-531035LegendNo ratings yet
- CPC CornerDocument5 pagesCPC Cornereduardo perez ramirezNo ratings yet
- Jurnal 1 PDFDocument8 pagesJurnal 1 PDFDhyan Hardiyanti BaharNo ratings yet
- Patient-Centered Pharmacy CommunicationDocument51 pagesPatient-Centered Pharmacy Communicationribka sparkleNo ratings yet
- Prabavathi.u Inter-Relation Between Clinical Name ChangedDocument63 pagesPrabavathi.u Inter-Relation Between Clinical Name ChangedVenkatram PrabhuNo ratings yet
- The Doctor-Patient RelationshipDocument55 pagesThe Doctor-Patient RelationshipMuhammad NaveedNo ratings yet
- GoodPractice WS DignityDocument3 pagesGoodPractice WS DignityGabriella RezmüvesNo ratings yet
- Doctor - Patient RelationshipDocument32 pagesDoctor - Patient RelationshipRushdaNo ratings yet
- Developing A Psychiatrist - Patient Relationship When Both People Are Doctors: A Qualitative StudyDocument10 pagesDeveloping A Psychiatrist - Patient Relationship When Both People Are Doctors: A Qualitative Studymasyi wimy johandhikaNo ratings yet
- Psychiatric Nursing Care Plans: Interventions for DepressionDocument6 pagesPsychiatric Nursing Care Plans: Interventions for DepressionCarmen Angela DusaranNo ratings yet
- HHS Public Access: Caregiver, Patient, and Nurse Visit Communication Patterns in Cancer Home HospiceDocument17 pagesHHS Public Access: Caregiver, Patient, and Nurse Visit Communication Patterns in Cancer Home HospiceRatih puspita DewiNo ratings yet
- Comunica Ting With PsychoticsDocument3 pagesComunica Ting With PsychoticsC. B.No ratings yet
- Doctor-Patient Relationship: "A Research Assignment - Mohamed Abdulhafeez"Document6 pagesDoctor-Patient Relationship: "A Research Assignment - Mohamed Abdulhafeez"AmiiinNo ratings yet
- Doctor-Patient Relationship: Hyacinth C. Manood, MD, FPPADocument25 pagesDoctor-Patient Relationship: Hyacinth C. Manood, MD, FPPAmr_davidNo ratings yet
- Doctor-Patient Communication A ReviewDocument6 pagesDoctor-Patient Communication A ReviewWagiono SuparanNo ratings yet
- Impact of Nurse-Patient Relationship On Quality of Care and Patient Autonomy in Decision-MakingDocument24 pagesImpact of Nurse-Patient Relationship On Quality of Care and Patient Autonomy in Decision-MakingMary LowryNo ratings yet
- Successful Doctor Patient Communication PDFDocument6 pagesSuccessful Doctor Patient Communication PDFMak Alisson BorgesNo ratings yet
- Doctor-Patient Communication ReviewDocument8 pagesDoctor-Patient Communication ReviewJAKE BENZYN TENo ratings yet
- Group Assignment 6.Document21 pagesGroup Assignment 6.Putri PrajaNo ratings yet
- Tugas BHP Hub Pasien DokterDocument14 pagesTugas BHP Hub Pasien DokterJoelNo ratings yet
- Interventions To Enhance Communication Among Patients, Providers, and FamiliesDocument8 pagesInterventions To Enhance Communication Among Patients, Providers, and FamiliesvabcunhaNo ratings yet
- Patient Practitioner Relationship 1Document24 pagesPatient Practitioner Relationship 1Dr Aniqa SundasNo ratings yet
- Everyday Ethics in An Acute Psychiatric UnitDocument4 pagesEveryday Ethics in An Acute Psychiatric Unitsetya indahNo ratings yet
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel AdlyNo ratings yet
- Unit 3 Final DraftDocument13 pagesUnit 3 Final Draftapi-252312023No ratings yet
- 114RLE JReading LagudaDocument3 pages114RLE JReading LagudaKayeNo ratings yet
- Health Communication Models Improve Patient OutcomesDocument27 pagesHealth Communication Models Improve Patient OutcomesJeffrey SuNo ratings yet
- Health Care in Custody: Ethical Fundamentals: Hans Wolff, Alejandra Casillas, Jean-Pierre Rieder, Laurent GétazDocument7 pagesHealth Care in Custody: Ethical Fundamentals: Hans Wolff, Alejandra Casillas, Jean-Pierre Rieder, Laurent GétazRoman Al MamunNo ratings yet
- Four Models of the Physician-Patient RelationshipDocument14 pagesFour Models of the Physician-Patient RelationshipcarmenNo ratings yet
- Profesionalismo MedicoDocument15 pagesProfesionalismo MedicoR4pT0r666No ratings yet
- Revised ThesisDocument27 pagesRevised ThesisAira FrancescaNo ratings yet
- Wampold, 2015 - How - Important - Are - The - Common - FactorsDocument6 pagesWampold, 2015 - How - Important - Are - The - Common - Factorsup201900768No ratings yet
- Boa Comunicação (BMJ02) PDFDocument4 pagesBoa Comunicação (BMJ02) PDFJonas NascimentoNo ratings yet
- How Important Are The Common Factors in Psychotherapy? An UpdateDocument8 pagesHow Important Are The Common Factors in Psychotherapy? An UpdateCoordinacionPsicologiaVizcayaGuaymasNo ratings yet
- Introduction to the Patient Interview. Introduction to Psychiatry . Preclinical Foundations and Clinical Essentials (pp. 38–69).Document32 pagesIntroduction to the Patient Interview. Introduction to Psychiatry . Preclinical Foundations and Clinical Essentials (pp. 38–69).Aline RangelNo ratings yet
- The Doctor Patient Relationship PDFDocument8 pagesThe Doctor Patient Relationship PDFWagiono Suparan100% (2)
- The Role of PhysiciansDocument5 pagesThe Role of PhysiciansMarvin ThomasNo ratings yet
- The History of Patient-Centered InterviewingDocument12 pagesThe History of Patient-Centered Interviewingbencleese100% (1)
- AMI Toolkit Conversation GuideDocument8 pagesAMI Toolkit Conversation GuideZohrahLiaqatNo ratings yet
- Patient Centerd CareDocument42 pagesPatient Centerd Care21910589No ratings yet
- Autonomy, HospitalityDocument12 pagesAutonomy, HospitalityDr. Mohammed SayedNo ratings yet
- Doctor Patient Communication: Yasir Irafat GROUP: 11 4 Semester Submitted To: Svetlana AbdikaimovaDocument14 pagesDoctor Patient Communication: Yasir Irafat GROUP: 11 4 Semester Submitted To: Svetlana AbdikaimovaYasir IrafatNo ratings yet
- Analysis: Empathic Responses in Clinical Practice: Intuition or Tuition?Document3 pagesAnalysis: Empathic Responses in Clinical Practice: Intuition or Tuition?piah89No ratings yet
- The Enduring and Evolving Nature of The Patient-PhysicianDocument11 pagesThe Enduring and Evolving Nature of The Patient-PhysicianSYLVIA RAMIS ASENJONo ratings yet
- Interpersonal CommunicationDocument5 pagesInterpersonal CommunicationSharwan KumawatNo ratings yet
- Pharmacy Level Iii NTQF Level - III: Learning Guide #0Document23 pagesPharmacy Level Iii NTQF Level - III: Learning Guide #0Samuel Merga100% (3)
- Empowerment and Serius Mental Illness-02Document12 pagesEmpowerment and Serius Mental Illness-02pepe pinitoNo ratings yet
- A Medical Director's Perspective: Understanding The Physician PerspectiveDocument3 pagesA Medical Director's Perspective: Understanding The Physician Perspectiveacma2010No ratings yet
- Connecting With Chronically Ill Patients To Improve Treatment AdherenceDocument2 pagesConnecting With Chronically Ill Patients To Improve Treatment AdherenceIdi FaithNo ratings yet
- Ethical Dilemmas in Nursing PDFDocument5 pagesEthical Dilemmas in Nursing PDFtitiNo ratings yet
- Doctor-Patient Communication: A Review of The LiteratureDocument16 pagesDoctor-Patient Communication: A Review of The LiteraturenutoNo ratings yet
- Relationship Centered CareDocument6 pagesRelationship Centered CareMeteoric8No ratings yet
- Q1: Define Medical Sociology and Its Scope: Medical SociologyDocument2 pagesQ1: Define Medical Sociology and Its Scope: Medical Sociologyhina rasoolNo ratings yet
- An Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDocument6 pagesAn Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDaria MoldovianNo ratings yet
- Common Factors + DefinitionDocument8 pagesCommon Factors + DefinitionVal AvivNo ratings yet
- Topic 5 - Doc Patient RelationshipDocument42 pagesTopic 5 - Doc Patient RelationshipAzry IskandarNo ratings yet
- Values Patient CenteredDocument4 pagesValues Patient CenteredRachmat AnsyoriNo ratings yet
- Determinants of Caregiving Experiences and MentalDocument12 pagesDeterminants of Caregiving Experiences and MentalanasenNo ratings yet
- Adi Sankaracharya's VivekachudamaniDocument955 pagesAdi Sankaracharya's VivekachudamanivsballaNo ratings yet
- Impact of The Doctor-Patient RelationshipDocument24 pagesImpact of The Doctor-Patient Relationshipravi dadlani parasramNo ratings yet
- Jonardon Ganeri - Indian Philosophy - A Reader-Routledge - Taylor & Francis Group (2020)Document377 pagesJonardon Ganeri - Indian Philosophy - A Reader-Routledge - Taylor & Francis Group (2020)mrigankkashNo ratings yet
- An Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDocument6 pagesAn Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDaria MoldovianNo ratings yet
- 02 Vivekachudamani Volume 02Document356 pages02 Vivekachudamani Volume 02Monsieur WelchNo ratings yet
- 1956 The Models of The Doctor-Patient RelationshipDocument8 pages1956 The Models of The Doctor-Patient Relationshipravi dadlani parasramNo ratings yet
- Jonardon Ganeri - Indian Philosophy - A Reader-Routledge - Taylor & Francis Group (2020)Document377 pagesJonardon Ganeri - Indian Philosophy - A Reader-Routledge - Taylor & Francis Group (2020)mrigankkashNo ratings yet
- Sadhanas From Vivekachudamani Step by Step Approcah To The LordDocument135 pagesSadhanas From Vivekachudamani Step by Step Approcah To The Lordadi_sam100% (1)
- 01 VivekchudamaniDocument115 pages01 Vivekchudamaniravi dadlani parasramNo ratings yet
- Isayeva N. - Shankara and Indian Philosophy. - 1993Document296 pagesIsayeva N. - Shankara and Indian Philosophy. - 1993Drastr100% (1)
- Awareness of Dying Aldine 1965 PDFDocument159 pagesAwareness of Dying Aldine 1965 PDFdrNo ratings yet
- The Doctrine of MayaDocument164 pagesThe Doctrine of Mayasukubh100% (1)
- Discover Secrets of The HimalayaDocument237 pagesDiscover Secrets of The Himalaya33elefanti80% (5)
- MeetingsWithSagesAndSaints PDFDocument409 pagesMeetingsWithSagesAndSaints PDFPrasanna Srinivasa RaoNo ratings yet
- ThepathofthemastersDocument256 pagesThepathofthemastersseanweilandNo ratings yet
- April 21 NewsDocument2 pagesApril 21 Newsapi-498713529No ratings yet
- Panel FormatDocument22 pagesPanel FormatbalakaleesNo ratings yet
- How to Discuss Difficult TopicsDocument7 pagesHow to Discuss Difficult TopicsAung Myo BalaNo ratings yet
- Pearson R Activity 2Document2 pagesPearson R Activity 2Lavinia Delos SantosNo ratings yet
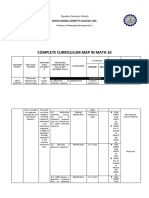
- Complete Curriculum Map in Math 10: Santa Maria Goretti College, IncDocument14 pagesComplete Curriculum Map in Math 10: Santa Maria Goretti College, IncArt Vincent Abenes AntiquinaNo ratings yet
- Theoretical FrameworkDocument2 pagesTheoretical FrameworkDhave Guibone Dela CruzNo ratings yet
- Health Information Management Profession: Real-World Case 1.1Document8 pagesHealth Information Management Profession: Real-World Case 1.1Yusra MehmoodNo ratings yet
- STD 2 SyllabusDocument6 pagesSTD 2 Syllabushweta173No ratings yet
- PMP Exam Prep Training BrochureDocument10 pagesPMP Exam Prep Training BrochureHarendra kumarNo ratings yet
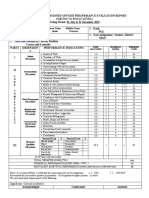
- Ratee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresDocument2 pagesRatee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresMeredith GalvezNo ratings yet
- 2021 2022 Spring HRM Assessment Brief 5Document6 pages2021 2022 Spring HRM Assessment Brief 5TrangNo ratings yet
- Caribbean Studies IaDocument16 pagesCaribbean Studies IaWayne Blackwood33% (6)
- Bns Accomplishment ReportDocument4 pagesBns Accomplishment ReportRaquel ParcareyNo ratings yet
- Research I Brief C - 2022-23Document3 pagesResearch I Brief C - 2022-23Vaishnavi PatilNo ratings yet
- Bus Terminal ThesisDocument5 pagesBus Terminal Thesisgjd6bfa4100% (2)
- 03 Goal-Use Analysis Worksheet-V2.0 (Excel)Document8 pages03 Goal-Use Analysis Worksheet-V2.0 (Excel)Alfredo FloresNo ratings yet
- Dualtech Training Center Presentation RVSADocument17 pagesDualtech Training Center Presentation RVSADennis SalongaNo ratings yet
- Instructions StorytellingDocument2 pagesInstructions StorytellingAzura W. ZakiNo ratings yet
- 1st-Exam 2019Document4 pages1st-Exam 2019Thanh LêNo ratings yet
- ABA in OBMDocument10 pagesABA in OBMQuésia CataldoNo ratings yet
- Soton Equity and Trusts - Seminar Materials 12-13 PDFDocument40 pagesSoton Equity and Trusts - Seminar Materials 12-13 PDFSam Kam100% (1)
- Deming 14 Point Almost DoneDocument13 pagesDeming 14 Point Almost DoneAda Ler100% (1)
- Skype Sex - Date of Birth - Nationality: Curriculum VitaeDocument4 pagesSkype Sex - Date of Birth - Nationality: Curriculum VitaeSasa DjurasNo ratings yet
- Enrolment Form - 2017 - Grade 10Document2 pagesEnrolment Form - 2017 - Grade 10Abed LowkeyNo ratings yet
- Codes StandardsDocument3 pagesCodes Standardsakshaf10No ratings yet
- Effects of Modular Learnings To StudentsDocument11 pagesEffects of Modular Learnings To StudentsSarmiento, Raphael M.No ratings yet
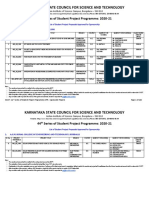
- 44S SPP Sanctioned Projects ListDocument240 pages44S SPP Sanctioned Projects ListM. Sadiq. A. PachapuriNo ratings yet
- Bs Coe Curriculum FlowchartDocument1 pageBs Coe Curriculum FlowchartRemi AltavaNo ratings yet
- Online Education Pros and ConsDocument7 pagesOnline Education Pros and ConstoralNo ratings yet
- Neurotransmitters - QuizizzDocument6 pagesNeurotransmitters - QuizizzushduNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)