0% found this document useful (0 votes)
101 views2 pagesEmployee Health Self-Check Form
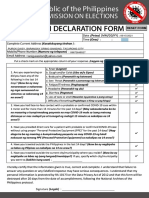
This document is an employee health declaration form used to screen employees for COVID-19 symptoms and exposure risks before starting a shift. It asks employees to check boxes indicating if they have symptoms like fever or cough, if they have had contact with a confirmed COVID-19 case, if they have provided direct care to a COVID-19 patient without protection, or if they have traveled outside the country or city in the last 14 days. It also authorizes the establishment to collect this health data for contact tracing and ensures the data will be kept private and destroyed after 30 days.
Uploaded by
TVni PotCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
101 views2 pagesEmployee Health Self-Check Form
This document is an employee health declaration form used to screen employees for COVID-19 symptoms and exposure risks before starting a shift. It asks employees to check boxes indicating if they have symptoms like fever or cough, if they have had contact with a confirmed COVID-19 case, if they have provided direct care to a COVID-19 patient without protection, or if they have traveled outside the country or city in the last 14 days. It also authorizes the establishment to collect this health data for contact tracing and ensures the data will be kept private and destroyed after 30 days.
Uploaded by
TVni PotCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd