You might also like
- CARAGA Passers Subprofessional CSE March 2023Document1 pageCARAGA Passers Subprofessional CSE March 2023PRC BoardNo ratings yet
- Salient Features of Republic Act 7160 - For MergeDocument10 pagesSalient Features of Republic Act 7160 - For Mergeanon_336606903100% (3)
- IHOMP Self Assessment ToolDocument7 pagesIHOMP Self Assessment ToolPhilip Duremdes Doromal80% (5)
- Tiktok Challenge Rules and Instructions:What Is The Challenge? Theme: Opm Hits (Filipino Artist)Document2 pagesTiktok Challenge Rules and Instructions:What Is The Challenge? Theme: Opm Hits (Filipino Artist)Dafchen Nio Mahasol100% (1)
- Relief From Accountability Sample Letter of StudentDocument8 pagesRelief From Accountability Sample Letter of StudentShiela ShieshielaNo ratings yet
- CS Form No. 7 Clearance FormDocument6 pagesCS Form No. 7 Clearance FormBenedict Van Velasco83% (12)
- Information Officer Duties Ra 7160Document2 pagesInformation Officer Duties Ra 7160RoseMantupar0% (1)
- Mtech822 AlphaDocument36 pagesMtech822 AlphaRapplerNo ratings yet
- Moa AmbulanceDocument4 pagesMoa AmbulanceJordan MB100% (1)
- Income Declaration FormDocument1 pageIncome Declaration FormGamy Glazyle100% (1)
- FINAL IPCR Kuya ErwinDocument3 pagesFINAL IPCR Kuya ErwinAilsa Craig100% (1)
- Of of of Of: Republic The PhilippinesDocument53 pagesOf of of Of: Republic The PhilippinesBoni Magtibay100% (3)
- Fact-Finding Investigation Conducted by The DILG - Duterte-CarpioDocument18 pagesFact-Finding Investigation Conducted by The DILG - Duterte-CarpioFrancis June Ygot100% (5)
- DepEd Bataan letter of introduction for teacher opening bank accountDocument1 pageDepEd Bataan letter of introduction for teacher opening bank accountJanet Cajes0% (2)
- Transmutation TableDocument152 pagesTransmutation TableEmil SayseNo ratings yet
- PRC Application for Crediting Self-Directed LearningDocument2 pagesPRC Application for Crediting Self-Directed LearningMarcus McWile MorningstarNo ratings yet
- Memorandum ReceiptDocument2 pagesMemorandum ReceiptSharmaine Valenzuela93% (15)
- IPCRDocument42 pagesIPCRAnne Secretbox73% (22)
- A U T H o R I Z A T I o N L e T T e R Sample For CenomarDocument2 pagesA U T H o R I Z A T I o N L e T T e R Sample For CenomarJomz Magtibay87% (15)
- CS Form No. 4 Certification of Assumption To DutyDocument1 pageCS Form No. 4 Certification of Assumption To DutyRic Laurence Sayson67% (6)
- PRC Application for Crediting CPD ActivitiesDocument2 pagesPRC Application for Crediting CPD ActivitiesJerwin Cases Tiamson100% (3)
- Schools Omnibus Certificate of Compliance: Depedro13-Rec-004/R3/2-18-2020Document2 pagesSchools Omnibus Certificate of Compliance: Depedro13-Rec-004/R3/2-18-2020Center for Healthcare ProfessionsNo ratings yet
- CHED Administrative Order (AO) No. 6, Series of 2014Document5 pagesCHED Administrative Order (AO) No. 6, Series of 2014Joedel Peñaranda100% (1)
- CPCS For GOCCDocument63 pagesCPCS For GOCCimianmorales57% (7)
- Pass SlipDocument4 pagesPass SlipMalou Mico CastilloNo ratings yet
- Test-Drill Examination Answer SheetDocument1 pageTest-Drill Examination Answer SheetPaul Christian P. Santos, RN75% (8)
- Guidelines and Implementing RulesDocument1 pageGuidelines and Implementing RulesDonita Rose Najera Nuestro67% (3)
- Supreme Court of The Philippines: List of Successful ExamineesDocument68 pagesSupreme Court of The Philippines: List of Successful ExamineesPRC Board94% (18)
- Health DeclarationDocument1 pageHealth DeclarationVanessa MendezNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNrc A.No ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormVladd DreiNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - AMARCK JOHN EUSTAQUIONo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formralph sabaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormFedelyn SemenianoNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- FOE Examinee's GuideDocument1 pageFOE Examinee's GuideNOOB 100No ratings yet
- Manual On Administering Civil Service Examination - Pen & Paper TestDocument1 pageManual On Administering Civil Service Examination - Pen & Paper TestJunette PaguioNo ratings yet
- Health Checklist: Question / Tanong Yes NoDocument1 pageHealth Checklist: Question / Tanong Yes NoKiel BalancioNo ratings yet
- Health Declaration Form - 2022-05 Revised (A5)Document1 pageHealth Declaration Form - 2022-05 Revised (A5)TOPNOTCHER PhilippinesNo ratings yet
- Health Declaration Form 2022 05 Revised A5Document1 pageHealth Declaration Form 2022 05 Revised A5Lyric'sMusicalNo ratings yet
- Health Declaration Form - A1 (Whole Page) - A (1) (PDF - Io)Document2 pagesHealth Declaration Form - A1 (Whole Page) - A (1) (PDF - Io)LET ME THINKNo ratings yet
- Health Declaration Form 1Document2 pagesHealth Declaration Form 1Elorde M. ShalaniNo ratings yet
- Camaman-an National High School Health ChecklistDocument1 pageCamaman-an National High School Health ChecklistTristan BabaylanNo ratings yet
- Health-Declaration-Form 2Document1 pageHealth-Declaration-Form 2menchieNo ratings yet
- Health Form for School EntryDocument1 pageHealth Form for School Entryargie joy marieNo ratings yet
- 2021 0202 Health Checklist Disclosure FormDocument2 pages2021 0202 Health Checklist Disclosure FormLea PacturanNo ratings yet
- Are You Experiencing: (Nakakaranas Ka Ba NG:) : Signature: - DateDocument1 pageAre You Experiencing: (Nakakaranas Ka Ba NG:) : Signature: - Datechen moradaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlexander IgasanNo ratings yet
- Health Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Document1 pageHealth Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Jhon Micheal AlicandoNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - ASharme Cagalawan AmahanNo ratings yet
- Health Checklist: Street, Barangay, District & CityDocument1 pageHealth Checklist: Street, Barangay, District & CityZula DapugoNo ratings yet
- Health Declaration Health Declaration: Body Temperature: - Body TemperatureDocument1 pageHealth Declaration Health Declaration: Body Temperature: - Body TemperatureRexenne BenigaNo ratings yet
- Revised Health Declaration FormDocument1 pageRevised Health Declaration FormMei SasucaNo ratings yet
- CECILIO APOSTOL ELEMENTARY HEALTH CHECKDocument1 pageCECILIO APOSTOL ELEMENTARY HEALTH CHECKMikoy Fordan AntolinoNo ratings yet
- Health Checklist Employees 1 Converted 1Document2 pagesHealth Checklist Employees 1 Converted 1the7thAliceNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAaron FlorentinoNo ratings yet
- Region 3 - 08202023 List of Passers SubDocument18 pagesRegion 3 - 08202023 List of Passers SubTheSummitExpressNo ratings yet
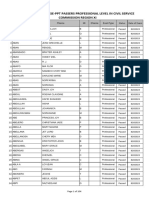
- R3 - List of Passers - 08202023 Pro - ForDocument103 pagesR3 - List of Passers - 08202023 Pro - ForTOPNOTCHER Philippines100% (1)
- Sub August 2023Document7 pagesSub August 2023TOPNOTCHER PhilippinesNo ratings yet
- 13 - 08202023 List of Passers SubDocument44 pages13 - 08202023 List of Passers SubTOPNOTCHER PhilippinesNo ratings yet
- R13 - List of Passers - 08202023 Pro - ForDocument234 pagesR13 - List of Passers - 08202023 Pro - ForTOPNOTCHER Philippines67% (3)
- 08202023cseppt Prof PasserDocument104 pages08202023cseppt Prof PasserTOPNOTCHER Philippines100% (2)
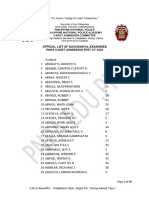
- Pnpacat Passes 1Document42 pagesPnpacat Passes 1TOPNOTCHER PhilippinesNo ratings yet
- R9 PROF-List of Passers 08-20-2023Document25 pagesR9 PROF-List of Passers 08-20-2023TOPNOTCHER Philippines100% (5)
- Prof August 2023Document47 pagesProf August 2023TOPNOTCHER PhilippinesNo ratings yet
- DOST 2023 QualifiersDocument251 pagesDOST 2023 QualifiersTOPNOTCHER Philippines100% (2)
- R9 SUBPROF-List of Passers 08-20-2023Document2 pagesR9 SUBPROF-List of Passers 08-20-2023TOPNOTCHER PhilippinesNo ratings yet
- R8 List of Passers 08202023 ProfessionalDocument32 pagesR8 List of Passers 08202023 ProfessionalTOPNOTCHER PhilippinesNo ratings yet
- 2022 JLSS QualifiersDocument36 pages2022 JLSS QualifiersTOPNOTCHER PhilippinesNo ratings yet
- Excuse Letter Template Sore EyesDocument1 pageExcuse Letter Template Sore EyesTOPNOTCHER Philippines0% (1)
- Final List 2023Document901 pagesFinal List 2023TOPNOTCHER Philippines67% (6)
- DOST 2023 QualifiersDocument251 pagesDOST 2023 QualifiersTOPNOTCHER Philippines100% (2)
- Final List 2023Document901 pagesFinal List 2023TOPNOTCHER Philippines67% (6)
- PMAVisayasDocument12 pagesPMAVisayasTOPNOTCHER PhilippinesNo ratings yet
- Pnpacat 2022 PassersDocument39 pagesPnpacat 2022 PassersTOPNOTCHER Philippines100% (1)
- Final List Pnpacat 2022Document752 pagesFinal List Pnpacat 2022TOPNOTCHER PhilippinesNo ratings yet
- March 26 Cse-Ppt Result NCRDocument468 pagesMarch 26 Cse-Ppt Result NCRTOPNOTCHER Philippines100% (1)
- Dost Sei Scholars 2022 2023Document199 pagesDost Sei Scholars 2022 2023TOPNOTCHER PhilippinesNo ratings yet
- Generic Application For PAFOC Class 2024 (18 April 2023)Document2 pagesGeneric Application For PAFOC Class 2024 (18 April 2023)TOPNOTCHER Philippines50% (2)
- Pnpacat 2021 PassersDocument29 pagesPnpacat 2021 PassersTOPNOTCHER Philippines100% (2)
- Health Declaration Form - 2022-05 Revised (A5)Document1 pageHealth Declaration Form - 2022-05 Revised (A5)TOPNOTCHER PhilippinesNo ratings yet
- PM A 2022 List MindanaoDocument39 pagesPM A 2022 List MindanaoTOPNOTCHER PhilippinesNo ratings yet
- PMAEE Passers 1Document3 pagesPMAEE Passers 1TOPNOTCHER PhilippinesNo ratings yet
- PMA Class of 2026Document3 pagesPMA Class of 2026TOPNOTCHER PhilippinesNo ratings yet
- Generic Application 18 Feb 2022 (For PAFOC and SPECIAL ENLISTMENT) .PDF#Pdfjs - Action DownloadDocument2 pagesGeneric Application 18 Feb 2022 (For PAFOC and SPECIAL ENLISTMENT) .PDF#Pdfjs - Action DownloadTOPNOTCHER Philippines83% (12)
- DOST-SEI Qualifiers 2021Document154 pagesDOST-SEI Qualifiers 2021TOPNOTCHER Philippines82% (11)
- Sacramento Steps Forward Fact Sheet Final 3.25Document2 pagesSacramento Steps Forward Fact Sheet Final 3.25Kris HooksNo ratings yet
- COVID19 HandbookDocument94 pagesCOVID19 HandbookRagavNo ratings yet
- Kent Bulloch, William Young Sr. ComplaintDocument33 pagesKent Bulloch, William Young Sr. ComplaintLaw&CrimeNo ratings yet
- Ancheta Et Al Handwashing - Chap4Document53 pagesAncheta Et Al Handwashing - Chap4Jaylord VerazonNo ratings yet
- European Journal of Pharmacology: Gayathri Krishna, Vinod Soman Pillai, Mohanan Valiya VeettilDocument11 pagesEuropean Journal of Pharmacology: Gayathri Krishna, Vinod Soman Pillai, Mohanan Valiya VeettilautomationenggNo ratings yet
- Executive Order 202-202.88 (January 4)Document182 pagesExecutive Order 202-202.88 (January 4)OANo ratings yet
- COVID-19 Live Updates: Total Number of Cases Passes 168 MillionDocument29 pagesCOVID-19 Live Updates: Total Number of Cases Passes 168 MillionXx XxNo ratings yet
- Shelter in PlaceDocument29 pagesShelter in PlaceCourtney-Ann Clarkin DelaneyNo ratings yet
- Kimberly.t.guidry@hawaii - Gov Robert.t.nakatsuji@hawaii - Gov Craig.y.iha@hawaii - Gov Michelle.l.agsalda@hawaii - GovDocument12 pagesKimberly.t.guidry@hawaii - Gov Robert.t.nakatsuji@hawaii - Gov Craig.y.iha@hawaii - Gov Michelle.l.agsalda@hawaii - GovHonolulu Star-AdvertiserNo ratings yet
- IQ4I Research & Consultancy Published A New Report On "Active Pharmaceutical Ingredient (API) Global Market - Forecast To 2027"Document7 pagesIQ4I Research & Consultancy Published A New Report On "Active Pharmaceutical Ingredient (API) Global Market - Forecast To 2027"VinayNo ratings yet
- 2020 Accelerating Development of SARS-CoV-2 Vaccines - The Role For Controlled Human Infection ModelsDocument4 pages2020 Accelerating Development of SARS-CoV-2 Vaccines - The Role For Controlled Human Infection Modelsalejandromfunes1749No ratings yet
- 1 Lecture - Observing The Language of Research, Campaigns, and AdvocaciesDocument51 pages1 Lecture - Observing The Language of Research, Campaigns, and AdvocaciesAligmat Gonzales83% (6)
- The Implementation of Modular Distance Learning in The Philippine Secondary Public SchoolsDocument10 pagesThe Implementation of Modular Distance Learning in The Philippine Secondary Public SchoolsMARYRUTH SEDEÑONo ratings yet
- Idsa Covid 19 GL Serology v1.0Document66 pagesIdsa Covid 19 GL Serology v1.0Max CamargoNo ratings yet
- 0 - Second Wave Covid 19 For Webinar KARS PERSI 24 April 2020 by DickyDocument26 pages0 - Second Wave Covid 19 For Webinar KARS PERSI 24 April 2020 by DickyGatot YuliantoNo ratings yet
- Kan Causal Conjuctions/sebab AkibatDocument2 pagesKan Causal Conjuctions/sebab AkibatNovia RamadhaniNo ratings yet
- Stop COVID (19) Cold - Dr. Mercola 2020Document17 pagesStop COVID (19) Cold - Dr. Mercola 2020petr18No ratings yet
- Impact of The COVID-19 Pandemic On Mental Health and Quality of Life Among Local Residents in Liaoning Province, China: A Cross-Sectional StudyDocument12 pagesImpact of The COVID-19 Pandemic On Mental Health and Quality of Life Among Local Residents in Liaoning Province, China: A Cross-Sectional StudyieykatalibNo ratings yet
- Module 5-7Document37 pagesModule 5-7Clifford Lachica100% (1)
- Activity 1 COVID-19 Safety ProtocolsDocument2 pagesActivity 1 COVID-19 Safety ProtocolsErica Z. AdugNo ratings yet
- (2021) Critical Review and Research Needs of Ozone Applications Related To Virus Inactivation Potential Implications For SARS CoV 2Document20 pages(2021) Critical Review and Research Needs of Ozone Applications Related To Virus Inactivation Potential Implications For SARS CoV 2Vu TranNo ratings yet
- Israeli People's CommitteeDocument6 pagesIsraeli People's CommitteeSarah WestallNo ratings yet
- KMITL English Exit ExamDocument6 pagesKMITL English Exit ExamNARAWITH PUTTHANo ratings yet
- Self-Based & Covid Questions InsightsDocument32 pagesSelf-Based & Covid Questions InsightsRishabh GuptaNo ratings yet
- DepEd issuances on COVID-19 responseDocument7 pagesDepEd issuances on COVID-19 responseEdward Parcon GolilaoNo ratings yet
- Guía Verbos Modales 2020Document14 pagesGuía Verbos Modales 2020Mauricio JimenezNo ratings yet
- Impact of Covid-19 on education in BangladeshDocument6 pagesImpact of Covid-19 on education in BangladeshNishit Acherzee PalashNo ratings yet
- Stay-Safe-at-Work-A2 Covid 19Document1 pageStay-Safe-at-Work-A2 Covid 19madmossyNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.1 EngDocument7 pagesWHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.1 EngChristianNo ratings yet
- USDA Grants Totaling $410,000 Awarded: Entities Receive Funding To Tackle COVID-19Document28 pagesUSDA Grants Totaling $410,000 Awarded: Entities Receive Funding To Tackle COVID-19houstonheraldNo ratings yet