You might also like
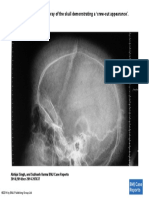
- Sagittal View of The X-Ray of The Skull Demonstrating A Crew-Cut Appearance'Document1 pageSagittal View of The X-Ray of The Skull Demonstrating A Crew-Cut Appearance'Ganesh HansdahNo ratings yet
- Sickle Cell and AnesthesiaDocument20 pagesSickle Cell and AnesthesiaGanesh HansdahNo ratings yet
- Heme SynthesisDocument51 pagesHeme SynthesisGanesh HansdahNo ratings yet
- Anesthetic Considerations in Porphyrias: Niels F. Jensen, Daniel S. Fiddler, MM, and Volker StriepeDocument9 pagesAnesthetic Considerations in Porphyrias: Niels F. Jensen, Daniel S. Fiddler, MM, and Volker StriepeGanesh HansdahNo ratings yet
- Sorry: Please Downloa DDocument1 pageSorry: Please Downloa DGanesh HansdahNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Rosewood Case AnalysisDocument5 pagesRosewood Case AnalysisJayant KushwahaNo ratings yet
- Democracy or Aristocracy?: Yasir MasoodDocument4 pagesDemocracy or Aristocracy?: Yasir MasoodAjmal KhanNo ratings yet
- Group Members: - Muhamad Sahli B Muda - Nurul Hana Balqis Baharom - Napsiah Abdul RahmanDocument18 pagesGroup Members: - Muhamad Sahli B Muda - Nurul Hana Balqis Baharom - Napsiah Abdul RahmanNurul Hana BalqisNo ratings yet
- Microsome S9 Prep ProtocolDocument22 pagesMicrosome S9 Prep ProtocolSAN912No ratings yet
- The Ethics of Peacebuilding PDFDocument201 pagesThe Ethics of Peacebuilding PDFTomas Kvedaras100% (2)
- S3 U4 MiniTestDocument3 pagesS3 U4 MiniTestĐinh Thị Thu HàNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesISMAEL KRIS DELA CRUZNo ratings yet
- Sub-Wings of YuvanjaliDocument2 pagesSub-Wings of Yuvanjalin_tapovan987100% (1)
- 1en 02 PDFDocument96 pages1en 02 PDFAndrey100% (2)
- All About TarlacDocument12 pagesAll About TarlacAnonymous uLb5vOjXNo ratings yet
- Chapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Document27 pagesChapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Masum ZamanNo ratings yet
- Exemption in Experience & Turnover CriteriaDocument4 pagesExemption in Experience & Turnover CriteriaVivek KumarNo ratings yet
- 全新全真题库一 PDFDocument36 pages全新全真题库一 PDFTzarlene100% (1)
- Case Study McsDocument4 pagesCase Study McsManjushree PatilNo ratings yet
- Industrial Motor Control Part IDocument38 pagesIndustrial Motor Control Part Ikibrom atsbha100% (2)
- Essay On Stem CellsDocument4 pagesEssay On Stem CellsAdrien G. S. WaldNo ratings yet
- Level I 2018 2019 Program Changes PDFDocument2 pagesLevel I 2018 2019 Program Changes PDFMuhammad BurairNo ratings yet
- Lesson 1 Concepts About Educational TechnologyDocument17 pagesLesson 1 Concepts About Educational TechnologyMarvin ContigaNo ratings yet
- Academic Performance of Senior High School Students 4Ps Beneficiaries in VNHSDocument19 pagesAcademic Performance of Senior High School Students 4Ps Beneficiaries in VNHSkathlen mae marollanoNo ratings yet
- AN44061A Panasonic Electronic Components Product DetailsDocument3 pagesAN44061A Panasonic Electronic Components Product DetailsAdam StariusNo ratings yet
- Chudamani Women Expecting ChangeDocument55 pagesChudamani Women Expecting ChangeMr AnantNo ratings yet
- Charles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)Document441 pagesCharles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)joan82% (17)
- Some Studies On Structure and Properties of Wrapped Jute (Parafil) YarnsDocument5 pagesSome Studies On Structure and Properties of Wrapped Jute (Parafil) YarnsVedant MahajanNo ratings yet
- Defining The Standards For Medical Grade Honey PDFDocument12 pagesDefining The Standards For Medical Grade Honey PDFLuis Alberto GarcíaNo ratings yet
- Richardson ResumeDocument3 pagesRichardson Resumeapi-549248694No ratings yet
- Final Quiz 2 - Attempt ReviewDocument6 pagesFinal Quiz 2 - Attempt Reviewkoraijohnson7No ratings yet
- High Speed Power TransferDocument33 pagesHigh Speed Power TransferJAYKUMAR SINGHNo ratings yet
- Lecture 7 - Friction - NptelDocument18 pagesLecture 7 - Friction - Nptels_murugan02No ratings yet
- Innocent Words That Make Her HornyDocument14 pagesInnocent Words That Make Her HornyH69% (13)
- Half Yearly Examination, 2017-18: MathematicsDocument7 pagesHalf Yearly Examination, 2017-18: MathematicsSusanket DuttaNo ratings yet