You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Harnoune Etc Al. - 2021 - BERT Based Clinical Knowledge Extraction For Biomedical Knowledge Graph Construction and AnalysisDocument12 pagesHarnoune Etc Al. - 2021 - BERT Based Clinical Knowledge Extraction For Biomedical Knowledge Graph Construction and AnalysisPrashantNo ratings yet
- An Overview of Metamap: Historical Perspective and Recent AdvancesDocument9 pagesAn Overview of Metamap: Historical Perspective and Recent AdvancesPrashantNo ratings yet
- Inst Titute Eofac Ctuar Ries O of Ind Dia: O Ffice O Order RDocument1 pageInst Titute Eofac Ctuar Ries O of Ind Dia: O Ffice O Order RPrashantNo ratings yet
- Actuarial Society of India: ExaminationsDocument5 pagesActuarial Society of India: ExaminationsPrashantNo ratings yet
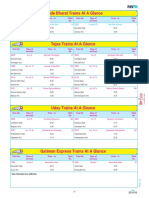
- Vande Bharat Trains at A Glance: 22435 Except M, TH Varanasi-New Delhi 1A 22436 Except M, TH New Delhi-Varanasi 1Document1 pageVande Bharat Trains at A Glance: 22435 Except M, TH Varanasi-New Delhi 1A 22436 Except M, TH New Delhi-Varanasi 1PrashantNo ratings yet
- Batman - The Dark Knight Returns 02 (Of 04) (1986)Document52 pagesBatman - The Dark Knight Returns 02 (Of 04) (1986)Prashant0% (1)
- Ai Ts SyllabusDocument3 pagesAi Ts SyllabusPrashantNo ratings yet
- Phase Topics 11th Class 1Document1 pagePhase Topics 11th Class 1PrashantNo ratings yet
- 1453372047general Organic ChemistryDocument12 pages1453372047general Organic ChemistryPrashantNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Learning From Students' Perception On Professors Through Opinion MiningDocument15 pagesLearning From Students' Perception On Professors Through Opinion MiningsulisNo ratings yet
- A Survey On Deep Learning For Named Entity RecognitionDocument20 pagesA Survey On Deep Learning For Named Entity RecognitionAhmad FajarNo ratings yet
- Spam Text Classification Using LSTM Recurrent Neural NetworkDocument5 pagesSpam Text Classification Using LSTM Recurrent Neural NetworkWARSE JournalsNo ratings yet
- Deep Learning Based Personality DetectionDocument6 pagesDeep Learning Based Personality DetectionJuan Flores MorocoNo ratings yet
- Simple Unsupervised Keyphrase Extraction Using Sentence EmbeddingsDocument9 pagesSimple Unsupervised Keyphrase Extraction Using Sentence EmbeddingsBekuma GudinaNo ratings yet
- Applications of Deep Learning To Sentiment Analysis of Movie ReviewsDocument8 pagesApplications of Deep Learning To Sentiment Analysis of Movie ReviewsTamara KomnenićNo ratings yet
- 1 PDFDocument28 pages1 PDFqaro kaduNo ratings yet
- 1904 08067Document68 pages1904 08067HiteshNo ratings yet
- World-GAN - A Generative Model For MinecraftDocument8 pagesWorld-GAN - A Generative Model For MinecraftGordonNo ratings yet
- Text-Mined Dataset of Inorganic Materials Synthesis Recipes: Data DescriptorDocument11 pagesText-Mined Dataset of Inorganic Materials Synthesis Recipes: Data Descriptornguyen van anNo ratings yet
- Social Network Hate Speech Detection For Amharic LanguageDocument15 pagesSocial Network Hate Speech Detection For Amharic LanguageCS & ITNo ratings yet
- Word 2 VecDocument6 pagesWord 2 Vecalihamda535No ratings yet
- Word Embeddings Master S ThesisDocument68 pagesWord Embeddings Master S ThesisAvishek JhaNo ratings yet
- Semantic Fake News Detection: A Machine Learning PerspectiveDocument12 pagesSemantic Fake News Detection: A Machine Learning PerspectiveNeha JainNo ratings yet
- AdvancedBooks - Python WikiDocument104 pagesAdvancedBooks - Python Wikisarvesh_mishra0% (1)
- 64 Natural Language Processing Interview Questions and Answers-18 Juli 2019Document30 pages64 Natural Language Processing Interview Questions and Answers-18 Juli 2019Ama AprilNo ratings yet
- GenAI - Text To ChartsDocument37 pagesGenAI - Text To ChartsRamesh KNo ratings yet
- Drug Recommendation SystemDocument7 pagesDrug Recommendation SystemRichard WaniNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewQaayed YusufNo ratings yet
- Senticnet 6: Ensemble Application of Symbolic and Subsymbolic Ai For Sentiment AnalysisDocument10 pagesSenticnet 6: Ensemble Application of Symbolic and Subsymbolic Ai For Sentiment AnalysisAleksandar CenicNo ratings yet
- Semantic Representations of Political Discourse Based On Topic Modeling and AlgorithmsDocument9 pagesSemantic Representations of Political Discourse Based On Topic Modeling and AlgorithmsInternational Journal of Innovative Science and Research Technology100% (1)
- A1 Engine SearchDocument2 pagesA1 Engine SearchMunthitra ThadthapongNo ratings yet
- Icpram 2020 38Document9 pagesIcpram 2020 38Melat FisshaNo ratings yet
- Model Klasifikasi Multi ClassDocument28 pagesModel Klasifikasi Multi ClassDonlot AjaNo ratings yet
- Word2vec Parameter Learning Explained: Xin Rong Ronxin@umich - EduDocument21 pagesWord2vec Parameter Learning Explained: Xin Rong Ronxin@umich - EduTryerNo ratings yet
- Us Presidential Vocabulary - IpynbDocument40 pagesUs Presidential Vocabulary - Ipynbbahadursoma3No ratings yet
- Language Modeling of Code-Mixed Text-1Document61 pagesLanguage Modeling of Code-Mixed Text-1sara chaoukiNo ratings yet
- CPT CodingDocument10 pagesCPT CodinghsyedamariaNo ratings yet
- Reading List and Presentation Schedule (CS 636 - Topics in Data Mining Research - Fall 2019-2020)Document3 pagesReading List and Presentation Schedule (CS 636 - Topics in Data Mining Research - Fall 2019-2020)Ahmed AnasNo ratings yet
- ProSOUL A Framework To Identify PropagandaFrom Online Urdu ContentDocument16 pagesProSOUL A Framework To Identify PropagandaFrom Online Urdu ContentBig DaddyNo ratings yet