You might also like
- Cad EhoDocument14 pagesCad EhomariakjaimesNo ratings yet
- Dislipidemias 2016Document72 pagesDislipidemias 2016mariakjaimesNo ratings yet
- Genitourinary Imaging in ChildrenDocument18 pagesGenitourinary Imaging in ChildrenmariakjaimesNo ratings yet
- Desordenes Del Desarrollo Sexual Copia 2Document16 pagesDesordenes Del Desarrollo Sexual Copia 2mariakjaimesNo ratings yet
- Antenatal and Perinatal Uro-NephrologyDocument7 pagesAntenatal and Perinatal Uro-NephrologymariakjaimesNo ratings yet
- Fetal ElectrocardiogramDocument5 pagesFetal ElectrocardiogrammariakjaimesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Fixation of Mandibular Fractures With 2.0 MM MiniplatesDocument7 pagesFixation of Mandibular Fractures With 2.0 MM MiniplatesRajan KarmakarNo ratings yet
- Pseudomonas Aeruginosa, 2013Document12 pagesPseudomonas Aeruginosa, 2013katiushikasNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakajhuvanNo ratings yet
- Spina BifidaDocument1 pageSpina BifidaM Isyhaduul IslamNo ratings yet
- CPG - Management of AcneDocument97 pagesCPG - Management of Acneumiraihana1No ratings yet
- Brachial PlexusDocument62 pagesBrachial PlexusTutankhamoun Akhenatoun100% (2)
- AtelectasisDocument9 pagesAtelectasisArni ZulsitaNo ratings yet
- List of Dental Colleges Issued Notification FOR THE YEAR 2017-18 AS ON 12.07.2017Document10 pagesList of Dental Colleges Issued Notification FOR THE YEAR 2017-18 AS ON 12.07.2017Shruthee KNo ratings yet
- DenturesDocument3 pagesDenturesMohammadNo ratings yet
- 2015 Article 110Document9 pages2015 Article 110Boleac HaralambieNo ratings yet
- A CDDocument54 pagesA CDDoc QueenieNo ratings yet
- Speman 056Document3 pagesSpeman 056mohd_ikrayemNo ratings yet
- Developmental AssessmentDocument3 pagesDevelopmental Assessmentsarguss14No ratings yet
- Cerebrospinal FluidDocument7 pagesCerebrospinal FluidjesusmsenatorNo ratings yet
- World Health OrganizationDocument2 pagesWorld Health OrganizationMarathi CalligraphyNo ratings yet
- RPT 54Document50 pagesRPT 54Leticia LopezNo ratings yet
- M3 Service ManualDocument115 pagesM3 Service ManualEmerson Gutiérrez CarrilloNo ratings yet
- Ifth DitionDocument25 pagesIfth DitionAlfie Omega0% (1)
- Dr.G.Thiruvenkadam Post Graduate Department of Pediatric & Preventive DentistryDocument55 pagesDr.G.Thiruvenkadam Post Graduate Department of Pediatric & Preventive Dentistryதிருவேங்கடம் கோபாலன்No ratings yet
- Infectious Diseases - Gorbach & Bartlett, 3E (2004)Document2,559 pagesInfectious Diseases - Gorbach & Bartlett, 3E (2004)Mădălina SuciuNo ratings yet
- NCV Findings in Lower LimbsDocument30 pagesNCV Findings in Lower LimbsKarthik BhashyamNo ratings yet
- Pediatric Acute Lymphoblastic LeukemiaDocument9 pagesPediatric Acute Lymphoblastic LeukemiaAlvin PratamaNo ratings yet
- Disaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Document23 pagesDisaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Clara EverlastNo ratings yet
- Cardiac Action PotentialDocument5 pagesCardiac Action PotentialjayNo ratings yet
- Physiology of Sleep: Michael Schupp MD FRCA Christopher D Hanning MD FRCADocument6 pagesPhysiology of Sleep: Michael Schupp MD FRCA Christopher D Hanning MD FRCArichie_ciandraNo ratings yet
- Appendix 13 - Green ListDocument17 pagesAppendix 13 - Green ListshaikhbilalroseNo ratings yet
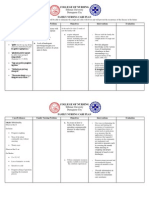
- FNCP - FinalDocument6 pagesFNCP - FinalmarkyabresNo ratings yet
- Oxygen and Carbon Dioxide TransportDocument9 pagesOxygen and Carbon Dioxide Transportpuchio100% (1)
- Type 2 Diabetes Final DraftDocument14 pagesType 2 Diabetes Final DraftAbbie HillsNo ratings yet
- Patellar Tendinitis Exercises - tcm28-180778Document5 pagesPatellar Tendinitis Exercises - tcm28-180778Maiko Gil HiwatigNo ratings yet