You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
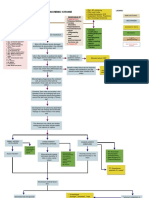
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lab 10 Blood and The HeartDocument7 pagesLab 10 Blood and The Heartharman parmarNo ratings yet
- 4 Stages of AnesthesiaDocument1 page4 Stages of AnesthesiaNURSES' PAD100% (8)
- ACLSDocument275 pagesACLSShajahan SideequeNo ratings yet
- Ayurveda in CADDocument3 pagesAyurveda in CADrajeevsonaliNo ratings yet
- SC PH 00362 - Jan9 - Empagliflozin Jardiance Module Update v5Document71 pagesSC PH 00362 - Jan9 - Empagliflozin Jardiance Module Update v5Jenny Calapati TorrijosNo ratings yet
- Elsevier Adaptive Quizzing - Quiz Performance ULTIMODocument18 pagesElsevier Adaptive Quizzing - Quiz Performance ULTIMOInteresante interNo ratings yet
- sureerat sua1,+ผู้จัดการวารสาร,+011วารสารหลอดเลือด+Volume+18+No2 2019 2019ThaiGuideline PDFDocument24 pagessureerat sua1,+ผู้จัดการวารสาร,+011วารสารหลอดเลือด+Volume+18+No2 2019 2019ThaiGuideline PDFThitipong NonnoiNo ratings yet
- Variante de Terminare A Arterei Carotide ExterneDocument5 pagesVariante de Terminare A Arterei Carotide ExterneCarolina HincuNo ratings yet
- Cardiac RehabDocument42 pagesCardiac RehabKapil LakhwaraNo ratings yet
- Q6 Cardiovascular PharmacologyDocument4 pagesQ6 Cardiovascular PharmacologyHainey GayleNo ratings yet
- Data Ibu Melahirkan Tahun 2019 Di Rsud Dok Ii Jayapura - NovemberDocument3 pagesData Ibu Melahirkan Tahun 2019 Di Rsud Dok Ii Jayapura - NovemberGALUHNo ratings yet
- Zoll AED PlusDocument5 pagesZoll AED PlusNurul FathiaNo ratings yet
- Strokeaha 116 013650Document7 pagesStrokeaha 116 013650priyaNo ratings yet
- Week4 FW04 Lecture SY19 20Document10 pagesWeek4 FW04 Lecture SY19 20Roy SisonNo ratings yet
- Bioassay of DigitalisDocument9 pagesBioassay of Digitalismahveen balochNo ratings yet
- ACHAI DLaboratory Actiivty 11 - The HeartDocument6 pagesACHAI DLaboratory Actiivty 11 - The HeartSYDNEY JILL ACHAINo ratings yet
- Preparing For The FRCS Tr+Orth Exam: Alex TrompeterDocument6 pagesPreparing For The FRCS Tr+Orth Exam: Alex Trompeterchu_chiang_3No ratings yet
- 6b. XII - MIPA - PROCEDURE TEXT - SSDocument5 pages6b. XII - MIPA - PROCEDURE TEXT - SSMuhammad Zidan IlhamiNo ratings yet
- J Jacadv 2022 100034Document14 pagesJ Jacadv 2022 100034Rui FonteNo ratings yet
- Sensus Icvcu 29.06.2022Document2 pagesSensus Icvcu 29.06.2022raka JantungunsNo ratings yet
- SINAS IDAI 2023 Flyer 2 Hal OK (PUTIH-Merah) - 281222Document2 pagesSINAS IDAI 2023 Flyer 2 Hal OK (PUTIH-Merah) - 281222izdihar rahmadindaNo ratings yet
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 pagesPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNo ratings yet
- Norepinephrine For Spinal Hypotension During Cesarean DeliveryDocument3 pagesNorepinephrine For Spinal Hypotension During Cesarean DeliveryANGELICANo ratings yet
- 2 - Holter ECG - TLC5000 Dynamic ECG SystemDocument3 pages2 - Holter ECG - TLC5000 Dynamic ECG SystemChristian Donfack fogang100% (1)
- Siemens Imaging AllDocument24 pagesSiemens Imaging AllVishnu0049No ratings yet
- Demo-Teaching DLP - MidayDocument10 pagesDemo-Teaching DLP - MidayCoLavs AvenueNo ratings yet
- Suspected Heart Failure: Section 5 Section 7 Section 8Document10 pagesSuspected Heart Failure: Section 5 Section 7 Section 8Javier TapiaNo ratings yet
- Manual Del TensiometroDocument58 pagesManual Del TensiometroHugo TrujilloNo ratings yet
- Health 9 q3 Week 1 2 Mod1 Udaundo Michelle KateDocument23 pagesHealth 9 q3 Week 1 2 Mod1 Udaundo Michelle KateRodman Ramiento100% (1)