You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Risk Assessment Registry SAMPLEDocument2 pagesRisk Assessment Registry SAMPLERTL JRNo ratings yet
- Impact of The Covid 19 Pandemic On TB Detection and Mortality in 2020Document8 pagesImpact of The Covid 19 Pandemic On TB Detection and Mortality in 2020Charles SandyNo ratings yet
- Community-Based Surveillance: A Scoping Review: BackgroundDocument25 pagesCommunity-Based Surveillance: A Scoping Review: BackgroundCharles SandyNo ratings yet
- Early COVID-19 Pandemic's Toll On Tuberculosis Services, WHO European Region, January To June 2020Document9 pagesEarly COVID-19 Pandemic's Toll On Tuberculosis Services, WHO European Region, January To June 2020Charles SandyNo ratings yet
- Health Statistics: Principles of Secondary Data AnalysisDocument61 pagesHealth Statistics: Principles of Secondary Data AnalysisCharles SandyNo ratings yet
- A Rush ADocument1 pageA Rush ACharles SandyNo ratings yet
- 1st PANDocument3 pages1st PANCharles SandyNo ratings yet
- 2023 GPB TemplateDocument26 pages2023 GPB Templatezandra cayabyabNo ratings yet
- Mini Research Hotel and TravelDocument20 pagesMini Research Hotel and Travellukman nurul hakimNo ratings yet
- La Batalla Por Tu MenteDocument2 pagesLa Batalla Por Tu MenteAda Milagros Meléndez DíazNo ratings yet
- Hygiene PolicyDocument4 pagesHygiene Policyprettyy chauhanNo ratings yet
- Letter - FL Region - Booster Healthcare Mandate 1-12-22Document2 pagesLetter - FL Region - Booster Healthcare Mandate 1-12-22Nick ReismanNo ratings yet
- TAFFIX SCIENCE PAPER Feb 2021Document10 pagesTAFFIX SCIENCE PAPER Feb 2021Sanja IlićNo ratings yet
- Reading and Writing SkillsDocument6 pagesReading and Writing SkillsAngela UntalanNo ratings yet
- Faisal ImranDocument2 pagesFaisal ImranSharjeel AhmedNo ratings yet
- Ahmed Et Al 2020 Epidemic of COVID-19Document7 pagesAhmed Et Al 2020 Epidemic of COVID-19Lauro Miranda DemenechNo ratings yet
- Chronic long-COVID Syndrome. A Protracted COVID-19 Illness With Neurological Dysfunctions 2021 PDFDocument4 pagesChronic long-COVID Syndrome. A Protracted COVID-19 Illness With Neurological Dysfunctions 2021 PDFRicardo Robles AlfaroNo ratings yet
- Bhert EO No. 3Document2 pagesBhert EO No. 3Ma Krystal Calimbo Evangelio - OntoNo ratings yet
- Barangay Employee Health Declaration FormDocument2 pagesBarangay Employee Health Declaration FormBarangay CentroNo ratings yet
- New CDC Mask GuidanceDocument1 pageNew CDC Mask GuidanceKristen Faith SchneiderNo ratings yet
- Rbi Attendant Admit LetterDocument4 pagesRbi Attendant Admit LetterNishant NarbhawarNo ratings yet
- Cesc Day3Document11 pagesCesc Day3Emily DayaNo ratings yet
- Robot CarDocument33 pagesRobot CarDalasa OljiraNo ratings yet
- BSPhar AY 2021-2022Document51 pagesBSPhar AY 2021-2022Crystal AnnNo ratings yet
- Mortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoDocument7 pagesMortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoM. Haseeb ShahzadNo ratings yet
- 4.2BSA - Acol, Angela F. - 4th Task - Ethics Worksheet - Option # 2Document10 pages4.2BSA - Acol, Angela F. - 4th Task - Ethics Worksheet - Option # 2Angela AcolNo ratings yet
- Nhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineDocument1 pageNhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccinePscual OuramdaneNo ratings yet
- Responsible Use of Media and Information During The COVID-19 PandemicDocument5 pagesResponsible Use of Media and Information During The COVID-19 PandemicTara Inada LaranjoNo ratings yet
- MutationDocument6 pagesMutationALEJANDRO COUTIÑO VALDOVINOSNo ratings yet
- Trial Registered Prospectively: Modification(s)Document6 pagesTrial Registered Prospectively: Modification(s)dincina70No ratings yet
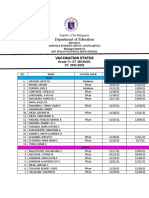
- Department of Education: Vaccination StatusDocument2 pagesDepartment of Education: Vaccination StatusKristelle BigawNo ratings yet
- EAPP Module Week 4Document8 pagesEAPP Module Week 4Aurora FontanillaNo ratings yet
- Mulnopiravir-FDA EUADocument10 pagesMulnopiravir-FDA EUAJaz ButuyanNo ratings yet
- Soal TO TOEFLDocument11 pagesSoal TO TOEFLIis AnnaNo ratings yet
- Health Declaration Form Health Declaration FormDocument1 pageHealth Declaration Form Health Declaration FormGerone NavaeraNo ratings yet
- Leimana Tara Rachel Returning To School PlanDocument16 pagesLeimana Tara Rachel Returning To School Planapi-524268535No ratings yet