You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (347)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lecture 06 - Tools and Techniques in BiotechnologyDocument162 pagesLecture 06 - Tools and Techniques in BiotechnologyAlkhair SangcopanNo ratings yet
- Biological Databases Lec 2,3Document49 pagesBiological Databases Lec 2,3najiullah khanNo ratings yet
- Peptide BondDocument2 pagesPeptide BondJENIFER PEARLINNo ratings yet
- DAVAO BiochemDocument5 pagesDAVAO BiochemVince Cabahug100% (1)
- Past Exam QuestionsDocument4 pagesPast Exam Questionskeirob100% (1)
- Microbiology A Systems Approach 5th Edition Cowan Test BankDocument39 pagesMicrobiology A Systems Approach 5th Edition Cowan Test Bankbanganwxy100% (31)
- Detection of Allergen Specific IgE Antibody ResponsesDocument12 pagesDetection of Allergen Specific IgE Antibody ResponsesYulius DonyNo ratings yet
- An Update On The Pathogenesis and Treatment of IgADocument12 pagesAn Update On The Pathogenesis and Treatment of IgAYulius DonyNo ratings yet
- Pediatric Hematology - Ask Hematologist - Understand HematologyDocument7 pagesPediatric Hematology - Ask Hematologist - Understand HematologyYulius DonyNo ratings yet
- Association Between Serum Albumin Level - Incidence of ESRD in Patients With IgA NephropathyDocument18 pagesAssociation Between Serum Albumin Level - Incidence of ESRD in Patients With IgA NephropathyYulius DonyNo ratings yet
- Follow-Up of DTC - What Should (And What Should Not) Be DoneDocument14 pagesFollow-Up of DTC - What Should (And What Should Not) Be DoneYulius DonyNo ratings yet
- A Review of The Role of Vitamins in Psoriasis in PregnancyDocument8 pagesA Review of The Role of Vitamins in Psoriasis in PregnancyYulius DonyNo ratings yet
- Vascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsDocument18 pagesVascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsYulius DonyNo ratings yet
- Piaa 065Document15 pagesPiaa 065Yulius DonyNo ratings yet
- (1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsDocument6 pages(1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsYulius DonyNo ratings yet
- Diabetes 1991 Baynes 405 12Document8 pagesDiabetes 1991 Baynes 405 12Yulius DonyNo ratings yet
- Exercise 1Document14 pagesExercise 1Michelle ViduyaNo ratings yet
- Factors Affecting Transposition of The Himar1 Mariner Transposon in VitroDocument9 pagesFactors Affecting Transposition of The Himar1 Mariner Transposon in VitroSubashini MuniandyNo ratings yet
- Genome, Transcriptome and Proteome PDFDocument17 pagesGenome, Transcriptome and Proteome PDFAdn CodeNo ratings yet
- Crispr Poster 2021Document4 pagesCrispr Poster 2021api-522847737No ratings yet
- TRANS PPT TOPIC - PlateletDocument4 pagesTRANS PPT TOPIC - PlateletPaul LesterNo ratings yet
- BY Sample Paper 7 UnsolvedDocument7 pagesBY Sample Paper 7 Unsolvedkookfics44No ratings yet
- 218 ภัทรดนัย ธูปสุวรรณ 7Document1 page218 ภัทรดนัย ธูปสุวรรณ 7Mr. ACDCNo ratings yet
- Uni ProtDocument6 pagesUni Protwilliam919No ratings yet
- Types of RespirationDocument5 pagesTypes of RespirationJevelyn Mendoza FarroNo ratings yet
- Pagination PHYMED 52238Document11 pagesPagination PHYMED 52238Dr. Kaushal Kishor SharmaNo ratings yet
- Nucleotide MetabolismDocument89 pagesNucleotide Metabolismfeby ary annasNo ratings yet
- K Biotech 123Document2 pagesK Biotech 123Dave DhruvNo ratings yet
- Protein Purification Problem SetDocument10 pagesProtein Purification Problem SetdhashrathNo ratings yet
- PROF ED. 213: Genetics: Cytological Bases of HeredityDocument40 pagesPROF ED. 213: Genetics: Cytological Bases of HeredityRonald DawalNo ratings yet
- Integrated Science Module 1 PDFDocument14 pagesIntegrated Science Module 1 PDFshieNo ratings yet
- Biotechnology: Quar TerDocument5 pagesBiotechnology: Quar TerShanaia Kaye Bais PamintuanNo ratings yet
- Crop LifeDocument7 pagesCrop Life유가연[학생](생명과학대학 유전생명공학과)No ratings yet
- Dr. Kunza Latif CV-with PicDocument3 pagesDr. Kunza Latif CV-with PicKunza LatifNo ratings yet
- Journal Of Biomedicine And Translational Research: Genetic Background of β Thalassemia Modifier: Recent UpdateDocument10 pagesJournal Of Biomedicine And Translational Research: Genetic Background of β Thalassemia Modifier: Recent Updatelantip rujitoNo ratings yet
- PCR Master Mix ProtocolDocument2 pagesPCR Master Mix ProtocolDo Thi Van AnhNo ratings yet
- Quiz On Enzyme KineticsDocument16 pagesQuiz On Enzyme Kineticschifunndo charlesNo ratings yet
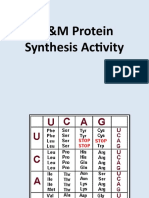
- MM Protein Synthesis Activity CBdiTEEDocument6 pagesMM Protein Synthesis Activity CBdiTEESHARIFAH BINTI HASSAN MoeNo ratings yet
- Chapter - 6 Molecular Basis of Inheritance - WatermarkDocument31 pagesChapter - 6 Molecular Basis of Inheritance - Watermarktejeshnaik026No ratings yet
- Alveolar Bone LossDocument10 pagesAlveolar Bone LossKhaled Al GhaebNo ratings yet