You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Biology Project-Drugs and Alcohol AbuseDocument23 pagesBiology Project-Drugs and Alcohol AbuseDeepika80% (20)
- 4.3.6 Are All Transplants The Same? NoDocument3 pages4.3.6 Are All Transplants The Same? NoZacary HarmonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NEMT6701278644Document5 pagesNEMT6701278644Dildar KhalilNo ratings yet
- ReportDocument2 pagesReportMuh ArafaNo ratings yet
- Love and Mental Health: IntimacyDocument2 pagesLove and Mental Health: IntimacyasdasdasdjdsdNo ratings yet
- Science 29 03 2024Document124 pagesScience 29 03 2024fernandopcaviniNo ratings yet
- Rahul K Ravindran - ProfileDocument1 pageRahul K Ravindran - ProfileRahul_Ravindra_2899No ratings yet
- Spice It For A Home Run!Document10 pagesSpice It For A Home Run!BeeHoof100% (1)
- Transmission of Dengue Hemorrhagic Fever in An Age Structured PopulationDocument13 pagesTransmission of Dengue Hemorrhagic Fever in An Age Structured PopulationRohan sharmaNo ratings yet
- Operational Guidelines For CeaDocument178 pagesOperational Guidelines For CeaNeelesh BhandariNo ratings yet
- Molecules 28 05022Document31 pagesMolecules 28 05022ela.sofiaNo ratings yet
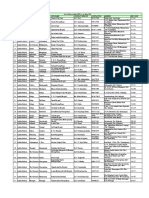
- List of Empannelled OPD's As On May 2010 S.No State District Location Opd Name Contact Person Contact No Address Pin CodeDocument89 pagesList of Empannelled OPD's As On May 2010 S.No State District Location Opd Name Contact Person Contact No Address Pin CodeSaurabh Saxena100% (1)
- Motivation TheoriesDocument15 pagesMotivation TheoriesMelNo ratings yet
- 2015 American Heart Association Guidelines Update For CPR and ECCDocument32 pages2015 American Heart Association Guidelines Update For CPR and ECCVauFauziah100% (2)
- Bliss Yoni Egg EbookDocument5 pagesBliss Yoni Egg EbookKaterina McCrimmon100% (1)
- Logical Framework Approach A Platform For Integrating The Mental Health and Nutritional Care For Controlling The Covid-19 PandemicDocument7 pagesLogical Framework Approach A Platform For Integrating The Mental Health and Nutritional Care For Controlling The Covid-19 PandemicAfiaa RgNo ratings yet
- Student - PPN 102 W24 Week 4 Nursing Process P1Document44 pagesStudent - PPN 102 W24 Week 4 Nursing Process P1phuongphuonganhanh171203No ratings yet
- Arab Fire Safety & Security Academy Arab Fire Safety & Security Academy Arab Fire Safety & Security Academy Arab Fire Safety & Security AcademyDocument1 pageArab Fire Safety & Security Academy Arab Fire Safety & Security Academy Arab Fire Safety & Security Academy Arab Fire Safety & Security AcademyMuhammad WaqasNo ratings yet
- BADACDocument8 pagesBADACdesiree joy corpuzNo ratings yet
- NCAPracticeExamCriminalLaw UPDATEDDocument9 pagesNCAPracticeExamCriminalLaw UPDATEDSanskriti NairNo ratings yet
- Understanding Cat Language - 50 Points - Aude YvanesDocument65 pagesUnderstanding Cat Language - 50 Points - Aude YvanesMJ FoustNo ratings yet
- Pune Hospital ListDocument48 pagesPune Hospital Listprakash kawadNo ratings yet
- Cityfheps Verification of Eligibility: 1. Referral SourceDocument2 pagesCityfheps Verification of Eligibility: 1. Referral SourceAbc FghNo ratings yet
- The Guardian Weekly - Vol. 209 No. 3 21 July 2023Document64 pagesThe Guardian Weekly - Vol. 209 No. 3 21 July 2023Observing MannNo ratings yet
- Construction Equipment Operations and Maintenance Pt.2Document13 pagesConstruction Equipment Operations and Maintenance Pt.2maryNo ratings yet
- Definition Essay On RespectDocument5 pagesDefinition Essay On Respectafibybflnwowtr100% (2)
- HospitalDocument20 pagesHospitalSparsh SharmaNo ratings yet
- 面源排放量推估手冊 PDFDocument228 pages面源排放量推估手冊 PDFTeresa ChenNo ratings yet
- Tirumala Tirupati Devasthanams (Official Booking Portal)Document1 pageTirumala Tirupati Devasthanams (Official Booking Portal)S SNo ratings yet
- Flange Managment ProcedureDocument47 pagesFlange Managment ProcedureIBRAHIMNo ratings yet