You might also like
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Open FractureDocument3 pagesOpen FractureDio AlexanderNo ratings yet
- Perioperative Assessment of the Maxillofacial Surgery Patient: Problem-based Patient ManagementFrom EverandPerioperative Assessment of the Maxillofacial Surgery Patient: Problem-based Patient ManagementElie M. FerneiniNo ratings yet
- The Management of Open Fracture: Gustillo RBDocument21 pagesThe Management of Open Fracture: Gustillo RBsagungw93No ratings yet
- Practice Guideline: Open Fracture: ObjectiveDocument2 pagesPractice Guideline: Open Fracture: ObjectiveIga AmanyzNo ratings yet
- 3) Singh2017Document5 pages3) Singh2017joteja8497No ratings yet
- Classification of Open FracturesDocument4 pagesClassification of Open FracturesAnderson DavidNo ratings yet
- Management of Lower Limb Trauma Open Wounds and FracturesDocument44 pagesManagement of Lower Limb Trauma Open Wounds and FracturesRumaicha ChachaNo ratings yet
- Open FractureDocument20 pagesOpen FracturegraceswanNo ratings yet
- Bedah Ortopedi 1. Open Fracture A. Gustillo-Anderson ClassificationDocument2 pagesBedah Ortopedi 1. Open Fracture A. Gustillo-Anderson ClassificationKarinaNo ratings yet
- Initial Assessment, Debridement, and Decision Making in The Salvage of Severely Injured Lower ExtremityDocument7 pagesInitial Assessment, Debridement, and Decision Making in The Salvage of Severely Injured Lower ExtremityVigneswaran VaradharajanNo ratings yet
- Antibiotic Use in Open FracturesDocument36 pagesAntibiotic Use in Open Fracturesapi-536775958No ratings yet
- LFTse PDFDocument43 pagesLFTse PDFNadia AlaydrusNo ratings yet
- Acute Management of Open Fractures: An Evidence-Based ReviewDocument23 pagesAcute Management of Open Fractures: An Evidence-Based ReviewerdiansyahzuldiNo ratings yet
- Principles of Management of Open FracturesDocument24 pagesPrinciples of Management of Open FracturesdhonnaNo ratings yet
- Presentasi PABI Pekanbaru 2021Document20 pagesPresentasi PABI Pekanbaru 2021raudhatul muttaqinNo ratings yet
- Manejo de Fracturas Expuestas 2020Document14 pagesManejo de Fracturas Expuestas 2020MARCELONo ratings yet
- Open FracturesDocument22 pagesOpen FracturesFerry RusdiansaputraNo ratings yet
- Open Fractures of The Long Bone: Herlambang B Mulyono, MDDocument52 pagesOpen Fractures of The Long Bone: Herlambang B Mulyono, MDalbertina tebayNo ratings yet
- Cement Beads and Cement Spa Indications,.3Document6 pagesCement Beads and Cement Spa Indications,.3Erika LlorenNo ratings yet
- Open Fractures TTBDocument45 pagesOpen Fractures TTBcromwellopoku42No ratings yet
- 222 PDFDocument2 pages222 PDFsumanth gowdaNo ratings yet
- Gustilo AndersonDocument14 pagesGustilo AndersonAditya PramanaNo ratings yet
- Open Fractures of The Lower Extremity: Current Management and Clinical OutcomesDocument10 pagesOpen Fractures of The Lower Extremity: Current Management and Clinical OutcomesSaffa AzharaaniNo ratings yet
- Open Fractures of The Lower Extremity PDFDocument10 pagesOpen Fractures of The Lower Extremity PDFmaudiaNo ratings yet
- Fractures: Principles and Problems of TreatmentDocument39 pagesFractures: Principles and Problems of Treatmentshulaihaw wan nur lubisNo ratings yet
- Open Fractures: DR Gourav RamukaDocument30 pagesOpen Fractures: DR Gourav RamukaGaurav Ramuka100% (1)
- Chapter 8 Provides The Following Information On Acute WoundsDocument7 pagesChapter 8 Provides The Following Information On Acute WoundsjoycefrancielleNo ratings yet
- Open FracturesDocument70 pagesOpen FracturesKelly Khesya100% (1)
- Open Fractures: Aga S. P. KetarenDocument43 pagesOpen Fractures: Aga S. P. KetarenErwin SiregarNo ratings yet
- Classification and ManagementDocument8 pagesClassification and ManagementFebry NdapaNo ratings yet
- 10.1097@00004623 197658040 00004Document6 pages10.1097@00004623 197658040 00004Edwin Alejandro Camacho GalueNo ratings yet
- Chuah, Bajuri, NorDocument5 pagesChuah, Bajuri, NorenggardiahNo ratings yet
- E W C O F: Arly Ound ARE IN PEN RacturesDocument3 pagesE W C O F: Arly Ound ARE IN PEN RacturesMatheis Laskar PelangiNo ratings yet
- Management of Open FracturesDocument89 pagesManagement of Open FracturesRoni YunartoNo ratings yet
- HindawiDocument5 pagesHindawiwijayantiNo ratings yet
- Prevencion en La Infeccion de Fractura ExpuestaDocument7 pagesPrevencion en La Infeccion de Fractura Expuestaalexi.garciaNo ratings yet
- Bone Repair Using The Masquelet TechniqueDocument13 pagesBone Repair Using The Masquelet TechniqueManny TantorNo ratings yet
- 2) Neelakandan2014Document14 pages2) Neelakandan2014joteja8497No ratings yet
- Zalavras 2017Document14 pagesZalavras 2017alexi.garciaNo ratings yet
- Management of Open FracturesDocument8 pagesManagement of Open FracturesAndreas KristianNo ratings yet
- Arthrodesis After Osteosynthesis and Infection of The Ankle JointDocument8 pagesArthrodesis After Osteosynthesis and Infection of The Ankle JointSeagate PramonoNo ratings yet
- Open Fractures and Damage ControlDocument35 pagesOpen Fractures and Damage ControlHamizi MD HanapiahNo ratings yet
- Wijaya Johanes Chendra, DR., SP - OTDocument41 pagesWijaya Johanes Chendra, DR., SP - OTRiqqah USNo ratings yet
- 97-506-1 Segundo CynDocument6 pages97-506-1 Segundo CynGalletita De JengibreNo ratings yet
- Wounds and Tissue RepairDocument4 pagesWounds and Tissue RepairMuhammad Mohsin Ali Dynamo0% (1)
- FX Abiertas Niños Timing 2005Document5 pagesFX Abiertas Niños Timing 2005Luigi Paolo Zapata DelgadoNo ratings yet
- Biological Approach For Managing Severe Gunshot Wounds: A Case ReportDocument5 pagesBiological Approach For Managing Severe Gunshot Wounds: A Case ReportHéctor Pando SánchezNo ratings yet
- Tibia-Open # MGDocument5 pagesTibia-Open # MGluckyariadneeNo ratings yet
- Fraktur Badan Tibia ShaftDocument10 pagesFraktur Badan Tibia ShaftQueenBalqisNo ratings yet
- Open Fractures: Complex Hand Injuries & ComplicationsDocument27 pagesOpen Fractures: Complex Hand Injuries & ComplicationsFelicianna Ashwinie StanleyNo ratings yet
- Injury: F. Lavini, C. Dall'Oca, S. Mezzari, T. Maluta, E. Luminari, F. Perusi, E. Vecchini, B. MagnanDocument6 pagesInjury: F. Lavini, C. Dall'Oca, S. Mezzari, T. Maluta, E. Luminari, F. Perusi, E. Vecchini, B. MagnanTefera LeteboNo ratings yet
- Gustilo Et AlDocument7 pagesGustilo Et Altan_yik_2No ratings yet
- Skills - Open Fracture ManagementDocument4 pagesSkills - Open Fracture ManagementFelixNo ratings yet
- UntitledDocument37 pagesUntitledYaser JasNo ratings yet
- Gustillo-Anderson Classification (Open - Fractures)Document1 pageGustillo-Anderson Classification (Open - Fractures)Fitriana Kusuma WardhaniNo ratings yet
- Orofacial Soft Tissue Injury and Wound HealingDocument38 pagesOrofacial Soft Tissue Injury and Wound HealingSabbir HossainNo ratings yet
- Initial Assessment and Management of Complex Forearm DefectsDocument14 pagesInitial Assessment and Management of Complex Forearm DefectsRoger Zambrana FloresNo ratings yet
- PBM Informe S7 2020 IDocument22 pagesPBM Informe S7 2020 Ivalery villegasNo ratings yet
- Open Fractures ProtocolDocument6 pagesOpen Fractures ProtocolKings PrideNo ratings yet
- Temporary Emergency Guidance To US Stroke Centers During The COVID-19 Pandemic On Behalf of The AHA/ASA Stroke Council LeadershipDocument6 pagesTemporary Emergency Guidance To US Stroke Centers During The COVID-19 Pandemic On Behalf of The AHA/ASA Stroke Council LeadershipVera VianaNo ratings yet
- Algo StrokeDocument2 pagesAlgo StrokeLocomotorica FK Uki100% (1)
- Best Practices in The Management of Orthopaedic Trauma: Acs TqipDocument38 pagesBest Practices in The Management of Orthopaedic Trauma: Acs TqipandhiyatnoermandakaNo ratings yet
- A Field Guide - Chapter 07Document16 pagesA Field Guide - Chapter 07andhiyatnoermandakaNo ratings yet
- EmbolizacionDocument8 pagesEmbolizacionnatalia.gallinoNo ratings yet
- Amelia Cruz ResumeDocument2 pagesAmelia Cruz Resumeapi-529343669No ratings yet
- Ravys ResumeDocument2 pagesRavys Resumeapi-332460214No ratings yet
- Su FentanylDocument28 pagesSu FentanylRyan GustomoNo ratings yet
- Cardiopulmonay Bypass 1Document1,203 pagesCardiopulmonay Bypass 1Dariel Muhammad Hegar SastrawigunaNo ratings yet
- Berg 2012Document7 pagesBerg 2012Mario Espinosa GamezNo ratings yet
- Cubierta Dental D-611 P.ideal C.P. 2Document4 pagesCubierta Dental D-611 P.ideal C.P. 2JessicaNo ratings yet
- Verken Lewenswetenskappe Graad 10 EksamenhersieningsboekDocument6 pagesVerken Lewenswetenskappe Graad 10 EksamenhersieningsboekSHANAAZ STEENKAMPNo ratings yet
- Nursing Care Plan Thyroid CancerDocument2 pagesNursing Care Plan Thyroid CancerKathleen DimacaliNo ratings yet
- Physiotherapy in Women After Breast Cancer Treatment - ReviewDocument7 pagesPhysiotherapy in Women After Breast Cancer Treatment - ReviewEmir BegagićNo ratings yet
- Pacemaker ThesisDocument4 pagesPacemaker Thesissandraarvesethsaltlakecity100% (2)
- Laporan Kasus SACG Dan Katarak Kongenital Pada AniridiaDocument15 pagesLaporan Kasus SACG Dan Katarak Kongenital Pada AniridiaIntan EkarulitaNo ratings yet
- Ko 2020Document48 pagesKo 2020npr00No ratings yet
- Focused Reviews: Bronchoscopic CryotherapyDocument11 pagesFocused Reviews: Bronchoscopic CryotherapyNEUMOLOGIA HNGAINo ratings yet
- IFU-Ortho - Reusable Surgical Instruments GB-Rev 6 - 240205 - 151904Document6 pagesIFU-Ortho - Reusable Surgical Instruments GB-Rev 6 - 240205 - 151904Lukas WijayantoNo ratings yet
- 2023 The Use of Zirconia For Implant-Supported Fixed Complete Dental Prostheses Narrative ReviewDocument14 pages2023 The Use of Zirconia For Implant-Supported Fixed Complete Dental Prostheses Narrative Reviewgerardo telloNo ratings yet
- CTG & FGG ComplicationDocument12 pagesCTG & FGG ComplicationmmputraNo ratings yet
- 1 s2.0 S0901502713000374 MainDocument8 pages1 s2.0 S0901502713000374 MainVeerawit LukkanasomboonNo ratings yet
- Plastic Surgeon Gets A Taste of His Own MedicineDocument9 pagesPlastic Surgeon Gets A Taste of His Own MedicineCarlos Eduardo AmorimNo ratings yet
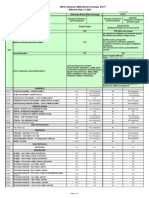
- Dental Fees Scale in Malaysia 2014Document1 pageDental Fees Scale in Malaysia 2014Arif Azizan100% (7)
- Dental Assistant Resume SampleDocument8 pagesDental Assistant Resume Samplef5e28dkq100% (2)
- Practical Point of Care Medical UltrasoundDocument199 pagesPractical Point of Care Medical Ultrasoundahmet kutluayNo ratings yet
- ACE PALAWAN MGAS-UPPER GROUND FLOOR-ModelDocument1 pageACE PALAWAN MGAS-UPPER GROUND FLOOR-ModelBerlin Andrew SionNo ratings yet
- Journal-Appraisal - Pgmi Del Prado, RockyDocument14 pagesJournal-Appraisal - Pgmi Del Prado, Rockyrockson del PradoNo ratings yet
- Comparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediaDocument6 pagesComparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediafatinfatharaniNo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- Alveolar Ridge Preservation Utilizing The Socket-Plug TechniqueDocument7 pagesAlveolar Ridge Preservation Utilizing The Socket-Plug Techniquekeily rodriguez100% (1)
- Jan Feb 2024Document124 pagesJan Feb 2024Gerardo Valenzuela GonzálezNo ratings yet
- AirSeal INGLESDocument60 pagesAirSeal INGLESPSC CAFAM CALLE 93No ratings yet
- Seminar: Treatment Planning in Orthodontic PatientsDocument105 pagesSeminar: Treatment Planning in Orthodontic PatientsVishal SharmaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)