You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Umbrella Effect of GICDocument11 pagesUmbrella Effect of GICLavanya Priya50% (4)
- TMJ AnkylosisDocument41 pagesTMJ AnkylosisSaritha DeviNo ratings yet
- Accelerated Osteogenic Orthodontics Technique: A 1-Stage Surgically Facilitated Rapid Orthodontic Technique With Alveolar AugmentationDocument11 pagesAccelerated Osteogenic Orthodontics Technique: A 1-Stage Surgically Facilitated Rapid Orthodontic Technique With Alveolar AugmentationMarcelaGutiérrezCarranzaNo ratings yet
- Susarla 2020Document8 pagesSusarla 2020MarcelaGutiérrezCarranzaNo ratings yet
- International Journal of Pediatric Otorhinolaryngology: Ryan H. Belcher, James D. Phillips TDocument5 pagesInternational Journal of Pediatric Otorhinolaryngology: Ryan H. Belcher, James D. Phillips TMarcelaGutiérrezCarranzaNo ratings yet
- Comprehensivepost Orthognathicsurgery Orthodontics: Complications, Misconceptions, and ManagementDocument17 pagesComprehensivepost Orthognathicsurgery Orthodontics: Complications, Misconceptions, and ManagementMarcelaGutiérrezCarranzaNo ratings yet
- Articulo 5Document7 pagesArticulo 5MarcelaGutiérrezCarranzaNo ratings yet
- Congenital Deformities and Developmental Abnormalities of The Mandibular Condyle in The Temporomandibular JointDocument8 pagesCongenital Deformities and Developmental Abnormalities of The Mandibular Condyle in The Temporomandibular JointMarcelaGutiérrezCarranzaNo ratings yet
- Dual Wavelength Spectrophotometry As A Diagnostic Test of The Pulp Chamber ContentsDocument7 pagesDual Wavelength Spectrophotometry As A Diagnostic Test of The Pulp Chamber Contentsl kkNo ratings yet
- Daftar Pustaka: Raisa Nadhifa, Dr. Drg. Ananto Ali Alhasyimi, M.DSC Drg. Niswati Fathmah Rosyida, M.DSCDocument4 pagesDaftar Pustaka: Raisa Nadhifa, Dr. Drg. Ananto Ali Alhasyimi, M.DSC Drg. Niswati Fathmah Rosyida, M.DSCAndrea Palleva WidjayaNo ratings yet
- Spring 2012Document32 pagesSpring 2012Roza NafilahNo ratings yet
- Marginal and Internal Fit of CADCAM Fabricated AllDocument3 pagesMarginal and Internal Fit of CADCAM Fabricated AllpoojaNo ratings yet
- Women in Dentistry Progress and ChallengesDocument16 pagesWomen in Dentistry Progress and ChallengesJaveriah YahyaNo ratings yet
- Hausmann 1974Document6 pagesHausmann 1974supriya bhartiNo ratings yet
- Egyptian Civilization's Contributions To Science and TechnologyDocument9 pagesEgyptian Civilization's Contributions To Science and TechnologyJalina, Emmanuel JoseNo ratings yet
- Bioceramics For Clinical Application in Regenerative DentistryDocument8 pagesBioceramics For Clinical Application in Regenerative DentistrypoojaNo ratings yet
- Glenoid Fossa RemodellingDocument59 pagesGlenoid Fossa RemodellingArnabNo ratings yet
- ITI Loading ProtocolsDocument5 pagesITI Loading ProtocolsnehaNo ratings yet
- Modified Wrap-Around RetainerDocument1 pageModified Wrap-Around RetainerJorge MelgarNo ratings yet
- Orthodontic Materials ListDocument27 pagesOrthodontic Materials ListsasitheunpluggedNo ratings yet
- Summary of Anatomy-1Document23 pagesSummary of Anatomy-1Omer AlsameiNo ratings yet
- Adaptaciones DesmostiliosDocument16 pagesAdaptaciones DesmostiliosMario Enrique GamarraNo ratings yet
- Early Childhood Caries: A ReviewDocument6 pagesEarly Childhood Caries: A ReviewGabriela MogaNo ratings yet
- Catholic University of America Student Health Plan For 2021-22 School YearDocument37 pagesCatholic University of America Student Health Plan For 2021-22 School YearThe College FixNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: ArticleDocument7 pagesMaxillofacial Defects and Their Classification: A Review.: ArticleVivek ShankarNo ratings yet
- Monolithic Solutions CHAIRSIDE: Instructions For UseDocument52 pagesMonolithic Solutions CHAIRSIDE: Instructions For UsemohammadNo ratings yet
- KIMART English ORTHOFREEDocument12 pagesKIMART English ORTHOFREEThuyNo ratings yet
- 2-External Root Resorption-J O ANDREASENDocument11 pages2-External Root Resorption-J O ANDREASENAlejandro morenoNo ratings yet
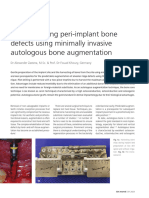
- The Bone Core Technique Reconstructing Peri Implant Bone Defects Using Minimally Invasive Autologous Bone AugmentationDocument6 pagesThe Bone Core Technique Reconstructing Peri Implant Bone Defects Using Minimally Invasive Autologous Bone AugmentationNamratha UmeshNo ratings yet
- Endodontic HistoryDocument4 pagesEndodontic HistoryJEAN BAILEY RAMOS ROXASNo ratings yet
- Asm 20030Document8 pagesAsm 20030preetvNo ratings yet
- Vol 5 Issue 4 - 07Document3 pagesVol 5 Issue 4 - 07Veysel OzerNo ratings yet
- Nasal and Facial Fractures: DR - Imran Qazi Ent A Tmo KTH PeshawarDocument42 pagesNasal and Facial Fractures: DR - Imran Qazi Ent A Tmo KTH Peshawarimran qaziNo ratings yet
- DIRECT FILLING GOLD RamDocument148 pagesDIRECT FILLING GOLD Ramrasagna reddyNo ratings yet
- Types of Balanced OcclusionDocument6 pagesTypes of Balanced Occlusionعلي صادق جعفرNo ratings yet
- Case 1 Dr. Beckett Dental OfficeDocument3 pagesCase 1 Dr. Beckett Dental OfficeTruc Nguyen ThanhNo ratings yet