You might also like
- Dermatology Essentials for Medical AssistantsFrom EverandDermatology Essentials for Medical AssistantsRating: 4 out of 5 stars4/5 (1)
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisFrom EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisNo ratings yet
- SkinDocument78 pagesSkinSamantha SansanoNo ratings yet
- Unit IV A. Physical AssessmentDocument129 pagesUnit IV A. Physical AssessmentGadez JeanpelNo ratings yet
- Chapter 013 SkinDocument65 pagesChapter 013 Skinoking4831No ratings yet
- Assessment of Skin, Hair and NailsDocument65 pagesAssessment of Skin, Hair and NailsVinzii Drt100% (1)
- Week 2 SKIN LHDDocument96 pagesWeek 2 SKIN LHDEloisa BrailleNo ratings yet
- Unit IV A. Physical AssessmentDocument129 pagesUnit IV A. Physical AssessmentJules Lorenz AbasoloNo ratings yet
- Nursing Assessment On Integumentary System: by Evelin MalintiDocument49 pagesNursing Assessment On Integumentary System: by Evelin Malintiwinda friyantiNo ratings yet
- Integumentary AssessmentDocument47 pagesIntegumentary AssessmentNesru Ahmed AkkichuNo ratings yet
- Health Assessment of The Integumentary SystemDocument5 pagesHealth Assessment of The Integumentary SystemA CNo ratings yet
- Chapter (6) Assessment of Skin, Hair and NailsDocument19 pagesChapter (6) Assessment of Skin, Hair and NailsSherlyn PedidaNo ratings yet
- UNIT - IV Assesment of Skin Head and NeckDocument48 pagesUNIT - IV Assesment of Skin Head and Neckraima ayazNo ratings yet
- Skills # 10: The Male Genitalia: Breast and Lymphatic VesselsDocument3 pagesSkills # 10: The Male Genitalia: Breast and Lymphatic VesselsAlyssa Ashley A. ImamNo ratings yet
- Types of Primary Skin LesionsDocument5 pagesTypes of Primary Skin LesionsKat TaasinNo ratings yet
- Skin Examination 1Document9 pagesSkin Examination 1Marry JuttNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- Physical Assessment - IntegumentDocument102 pagesPhysical Assessment - IntegumentDeeeeeNo ratings yet
- Chapter 26 Study GuideDocument7 pagesChapter 26 Study GuideTommie Ann LillpopNo ratings yet
- Pressure UlcerDocument66 pagesPressure UlcerSwarnkar JayeshNo ratings yet
- Assessment of SkinDocument22 pagesAssessment of SkinAzeemNo ratings yet
- Health Assessment 9Document16 pagesHealth Assessment 9shannon c. lewisNo ratings yet
- Assessment of SkinDocument11 pagesAssessment of SkinShreyas WalvekarNo ratings yet
- Dermatology TestsDocument6 pagesDermatology TestsLouise Alysson OrtegaNo ratings yet
- The Skin Hair and Nails Part 1 Anat and PhsyioDocument53 pagesThe Skin Hair and Nails Part 1 Anat and PhsyiomalvincayabyabNo ratings yet
- Nursing Care PlanDocument15 pagesNursing Care PlannicolealexandrakhoNo ratings yet
- Lect 4. Skin Hair and NailsDocument34 pagesLect 4. Skin Hair and Nailsdaniahisham05No ratings yet
- Integumentary DisorderDocument2 pagesIntegumentary DisorderFlappy GirlNo ratings yet
- Module 3 HomeworkDocument6 pagesModule 3 HomeworkCj LinceNo ratings yet
- NCM101 Lesson Guide 7Document28 pagesNCM101 Lesson Guide 7Yahra DatangNo ratings yet
- Skin AssessmentDocument50 pagesSkin AssessmentNayel ZeeshanNo ratings yet
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDocument7 pagesPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoNo ratings yet
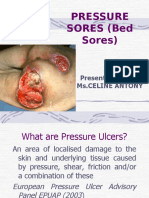
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDocument40 pagesPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiNo ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- 1.RagragPreventing Pressure Sore.1Document18 pages1.RagragPreventing Pressure Sore.1alsamixersNo ratings yet
- Physical AssessmentDocument19 pagesPhysical AssessmentMamerto Q. Flores IIINo ratings yet
- Assessing IntegumentaryDocument3 pagesAssessing IntegumentaryhectorNo ratings yet
- Health Assessment 1 - EENT (Lab)Document18 pagesHealth Assessment 1 - EENT (Lab)Reniella HidalgoNo ratings yet
- Skin. Hair Scalp and Nails With RationaleDocument3 pagesSkin. Hair Scalp and Nails With Rationalehatdog hatdogNo ratings yet
- Physical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NDocument20 pagesPhysical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NRyan Biwit100% (4)
- 1.skin Assessment & Diagnostic ProcedureDocument9 pages1.skin Assessment & Diagnostic Procedureyangi dokaNo ratings yet
- Skin An Essential Organ-IIDocument30 pagesSkin An Essential Organ-IIsameen tahirNo ratings yet
- Assessment of Skin, Hairs and NailsDocument85 pagesAssessment of Skin, Hairs and Nailsdileepkumar.duhs4817No ratings yet
- Tissue Integrity Outline Spring 2023Document25 pagesTissue Integrity Outline Spring 2023morganstorey0No ratings yet
- Technique of The Dermatologic Physical Examination: DiasDocument6 pagesTechnique of The Dermatologic Physical Examination: Diassylvia haryantoNo ratings yet
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaNo ratings yet
- Skin Care and Management of Pressure UlcerDocument24 pagesSkin Care and Management of Pressure UlcerchellczyNo ratings yet
- Image Gallery - Secondary Skin Lesions - Clinician's BriefDocument9 pagesImage Gallery - Secondary Skin Lesions - Clinician's BriefMabe AguirreNo ratings yet
- Script Skin Hairand Nail Assessment PDFDocument5 pagesScript Skin Hairand Nail Assessment PDFKolours KoloursNo ratings yet
- Wa0000.Document12 pagesWa0000.Florida ManNo ratings yet
- Skin Checklist ProcedureDocument6 pagesSkin Checklist ProcedureKristine Angie RamosNo ratings yet
- Wound Assessment & CareDocument32 pagesWound Assessment & Caresami siddiqNo ratings yet
- Skin-Hair-And-Nails-1 (20230308092246)Document26 pagesSkin-Hair-And-Nails-1 (20230308092246)Caramay S (2202111)No ratings yet
- Signs and Symptoms: Impaired Skin IntegrityDocument3 pagesSigns and Symptoms: Impaired Skin Integrityshadow gonzalezNo ratings yet
- SKINDocument12 pagesSKINJaleah Gwyneth Fernandez EdullantesNo ratings yet
- Assignment # 5: Integumentary System Explore: 1Document4 pagesAssignment # 5: Integumentary System Explore: 1Kassandra Shayne CaballeroNo ratings yet
- Safari - 26 Mar 2023, 11:28 AMDocument1 pageSafari - 26 Mar 2023, 11:28 AMErza KabashiNo ratings yet
- M. LepraeDocument22 pagesM. LepraeRina AlimuddinNo ratings yet
- Unit 3 Integumentary System Pathological ConditionsDocument43 pagesUnit 3 Integumentary System Pathological Conditionsalmira garciaNo ratings yet
- Cellulitis NCPDocument2 pagesCellulitis NCPKelly Riedinger85% (13)
- Next-Generation NCLEX Case Study For Gerontology in LPN/LVN Abuse and NeglectDocument3 pagesNext-Generation NCLEX Case Study For Gerontology in LPN/LVN Abuse and NeglectCrystal PughNo ratings yet
- Geriatric Functional Assessment: The Geriatric Review of SystemsDocument35 pagesGeriatric Functional Assessment: The Geriatric Review of SystemsNunu MirNo ratings yet
- Overview of AgingDocument17 pagesOverview of AgingCrystal PughNo ratings yet
- MARDocument1 pageMARCrystal PughNo ratings yet
- Theories of AgingDocument10 pagesTheories of AgingCrystal PughNo ratings yet
- Overview of AgingDocument17 pagesOverview of AgingCrystal PughNo ratings yet
- Chapter 3 The Skin, Hair, and NailsDocument1 pageChapter 3 The Skin, Hair, and NailsCrystal PughNo ratings yet
- Concept Map Template 1Document1 pageConcept Map Template 1Crystal PughNo ratings yet
- Blank Conceptual Care Map Handout Concept Mapping I Webinar 2-19Document2 pagesBlank Conceptual Care Map Handout Concept Mapping I Webinar 2-19Crystal PughNo ratings yet
- K EtaDocument14 pagesK EtaJosue Teni BeltetonNo ratings yet
- Dri InternshipDocument38 pagesDri InternshipGuruprasad Sanga100% (3)
- 2 Dawn150Document109 pages2 Dawn150kirubelNo ratings yet
- G1 Series User Manual Ver. 1.2Document101 pagesG1 Series User Manual Ver. 1.2unedo parhusip100% (1)
- How McDonald'sDocument2 pagesHow McDonald'spratik khandualNo ratings yet
- 3 Activities For Adults To Practice Modeling SELDocument10 pages3 Activities For Adults To Practice Modeling SELDavid Garcia PerezNo ratings yet
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDocument12 pagesAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991No ratings yet
- Dressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionDocument2 pagesDressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionAlvaCatalinaNo ratings yet
- Review - Practical Accounting 1Document2 pagesReview - Practical Accounting 1Kath LeynesNo ratings yet
- Case Study of Milk ProductionDocument46 pagesCase Study of Milk Productionmian21100% (2)
- FEM 3004 - Lab 10 Part 2editedDocument26 pagesFEM 3004 - Lab 10 Part 2editedAINA NADHIRAH BINTI A ROZEY / UPMNo ratings yet
- Project Management A Technicians Guide Staples TOCDocument5 pagesProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- IsoTherming® Hydroprocessing TechnologyDocument4 pagesIsoTherming® Hydroprocessing Technologyromi moriNo ratings yet
- Nta855 C400 D6 PDFDocument110 pagesNta855 C400 D6 PDFIsmael Grünhäuser100% (4)
- DPA Fact Sheet Women Prison and Drug War Jan2015 PDFDocument2 pagesDPA Fact Sheet Women Prison and Drug War Jan2015 PDFwebmaster@drugpolicy.orgNo ratings yet
- Adsorbents and Adsorption Processes For Pollution ControlDocument30 pagesAdsorbents and Adsorption Processes For Pollution ControlJoao MinhoNo ratings yet
- Alugbati Plant Pigment Extraction As Natural Watercolor SourceDocument6 pagesAlugbati Plant Pigment Extraction As Natural Watercolor SourceMike Arvin Serrano100% (1)
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Chapter 2 and 3 ImmunologyDocument16 pagesChapter 2 and 3 ImmunologyRevathyNo ratings yet
- Class Two Summer Vacation AssignmentDocument1 pageClass Two Summer Vacation AssignmentshahbazjamNo ratings yet
- Electri RelifDocument18 pagesElectri Relifsuleman247No ratings yet
- Funding HR2 Coalition LetterDocument3 pagesFunding HR2 Coalition LetterFox NewsNo ratings yet
- Task 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Document5 pagesTask 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Samir Mosquera-PalominoNo ratings yet
- Mainstreaming Gad Budget in The SDPDocument14 pagesMainstreaming Gad Budget in The SDPprecillaugartehalagoNo ratings yet
- Chemical Quick Guide PDFDocument1 pageChemical Quick Guide PDFAndrejs ZundaNo ratings yet
- Soil SSCDocument11 pagesSoil SSCvkjha623477No ratings yet
- Neurocisticercosis PDFDocument7 pagesNeurocisticercosis PDFFiorella Alexandra HRNo ratings yet
- Biopolymers: Overview of Several Properties and Consequences On Their ApplicationsDocument10 pagesBiopolymers: Overview of Several Properties and Consequences On Their ApplicationsrafacpereiraNo ratings yet
- Benzil PDFDocument5 pagesBenzil PDFAijaz NawazNo ratings yet
- Behavior Specific Praise Statements HandoutDocument3 pagesBehavior Specific Praise Statements HandoutDaniel BernalNo ratings yet