You might also like
- Borang Permohonan Cuti Clinic & PharmacyDocument1 pageBorang Permohonan Cuti Clinic & PharmacyectoclinicNo ratings yet
- Application of Leave FormDocument1 pageApplication of Leave FormbrendaluverNo ratings yet
- HR Leave Request FormDocument1 pageHR Leave Request FormFaraz Anwar AbroNo ratings yet
- Revised Company Loan FormDocument2 pagesRevised Company Loan FormAubrey UbayNo ratings yet
- DepEd Leave Application FormDocument2 pagesDepEd Leave Application FormJinn Dalisay Uy100% (3)
- Spredsheet format.docxDocument1 pageSpredsheet format.docxphungvcungNo ratings yet
- Personnel Action Notice: (PAN) Company NameDocument1 pagePersonnel Action Notice: (PAN) Company NamePaulNo ratings yet
- Leave FormDocument1 pageLeave FormbkgboqdraftsmanNo ratings yet
- Re Admission FormDocument2 pagesRe Admission FormMissy SamanthaNo ratings yet
- Authorization To DeductDocument1 pageAuthorization To Deductumanichole25No ratings yet
- LoanDocument1 pageLoanSunshine MoonlightNo ratings yet
- Form Employment Termination (631) - 2Document1 pageForm Employment Termination (631) - 2Mark VeederNo ratings yet
- Kami Export - Rop Job Application With Availability - Fillable For Website 1Document2 pagesKami Export - Rop Job Application With Availability - Fillable For Website 1api-459117525No ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-460289223No ratings yet
- Couples For Christ Couples For Christ: ( - HRS) ( - HRS) ( - HRS)Document2 pagesCouples For Christ Couples For Christ: ( - HRS) ( - HRS) ( - HRS)AlexgwapoNo ratings yet
- Applicant Endorsement FormDocument1 pageApplicant Endorsement Formliza avilaNo ratings yet
- Ic 38Document3 pagesIc 38Prasanth VedgarbNo ratings yet
- Leave Application Form WriteableDocument1 pageLeave Application Form WriteableBilly EresNo ratings yet
- Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word - Rop Job Application With Availablity Front-For Fillableapi-459900943No ratings yet
- Personnel Action Form TemplateDocument1 pagePersonnel Action Form TemplateHerbert BactongNo ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-460994161No ratings yet
- Leave Application 30-Dec-2022Document1 pageLeave Application 30-Dec-2022Faraz Anwar AbroNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormRashid MehmoodNo ratings yet
- Salary Deduction FormDocument1 pageSalary Deduction Formkrishneil kiritNo ratings yet
- Business Gateways International: Application For Leave/Permissions/On DutyDocument2 pagesBusiness Gateways International: Application For Leave/Permissions/On DutyinduNo ratings yet
- HRDF-0007Document1 pageHRDF-0007PrincessAntonetteDeCastroNo ratings yet
- Provident Fund Loan ApplicationDocument2 pagesProvident Fund Loan ApplicationRyahNeil Bohol MoralesNo ratings yet
- Clearance FormDocument1 pageClearance FormNaveen KumarNo ratings yet
- Clearance Form UpdatedDocument1 pageClearance Form UpdatedmarkanthonymailigNo ratings yet
- Leave Request FORMDocument1 pageLeave Request FORMCharlie GabalesNo ratings yet
- Housing Loan Application InsightsDocument4 pagesHousing Loan Application InsightsDebargha 2027No ratings yet
- Emergency Loan Request New FormatDocument2 pagesEmergency Loan Request New FormatAlyssa BayogNo ratings yet
- Membership FormDocument2 pagesMembership FormNick XiaoNo ratings yet
- The Information Given Will Be Treated in The Strictest ConfidenceDocument1 pageThe Information Given Will Be Treated in The Strictest ConfidenceGamini PereraNo ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-459924709No ratings yet
- Leave FormDocument1 pageLeave FormSudan ShresthaNo ratings yet
- 1-Annual Leave FormDocument2 pages1-Annual Leave FormmNo ratings yet
- 4 We Care Loan FormDocument2 pages4 We Care Loan FormJaneth ApatNo ratings yet
- Personnel FormDocument1 pagePersonnel Formclarisse.tdcNo ratings yet
- Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word - Rop Job Application With Availablity Front-For Fillableapi-459910112No ratings yet
- Job ApplicationDocument2 pagesJob Applicationapi-460349878No ratings yet
- Application For Family PensionDocument14 pagesApplication For Family PensionRashid NaeemNo ratings yet
- YeeeDocument2 pagesYeeeapi-459836987No ratings yet
- F&F SheetDocument3 pagesF&F SheetVikram KanojiyaNo ratings yet
- 05 Staff Loan ApplicationDocument2 pages05 Staff Loan ApplicationBernadette Sambrano EmbienNo ratings yet
- Less Than 12 Month Adjunct Ap: Account#Document1 pageLess Than 12 Month Adjunct Ap: Account#SushantNo ratings yet
- Leave FormDocument1 pageLeave FormKHIM JOSEPH MALICSENo ratings yet
- Authority To Deduct Form (ATD)Document1 pageAuthority To Deduct Form (ATD)Hr CPCINo ratings yet
- SBIapplicationformDocument5 pagesSBIapplicationformSufi DarweshNo ratings yet
- Payroll Deduction Authorization Form - 1Document1 pagePayroll Deduction Authorization Form - 1resar17_rgtNo ratings yet
- CPL FormDocument1 pageCPL FormElectrical jobNo ratings yet
- Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word - Rop Job Application With Availablity Front-For Fillableapi-461396148No ratings yet
- 2339 - EG FillableDocument1 page2339 - EG Fillablesherrif douchebagNo ratings yet
- LEAVE-REQUEST-FORM-Updated-03122024Document1 pageLEAVE-REQUEST-FORM-Updated-03122024michaelparnanesmaelNo ratings yet
- Syama Dynamic Engineering PVT LTD Leave Application Form: Date: Name of The EmployeeDocument1 pageSyama Dynamic Engineering PVT LTD Leave Application Form: Date: Name of The Employeejohnjune007No ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-459942138No ratings yet
- LuksDocument1 pageLukslaukesh chandNo ratings yet
- WORKER'S EMPLOYMENT CLEARANCEDocument4 pagesWORKER'S EMPLOYMENT CLEARANCEshayne rosanesNo ratings yet
- HR Associate Application FormDocument4 pagesHR Associate Application FormRobbin SinghNo ratings yet
- M885pes TMP1677 R1 31.12.2019Document1 pageM885pes TMP1677 R1 31.12.2019Thi HaNo ratings yet
- C885 - Pipe Jacking For Linkway To Entrance B: Layout PlanDocument1 pageC885 - Pipe Jacking For Linkway To Entrance B: Layout PlanThi HaNo ratings yet
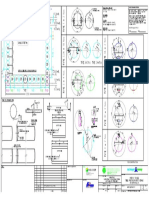
- M885pes TMP1674 R1 31.12.2019Document1 pageM885pes TMP1674 R1 31.12.2019Thi HaNo ratings yet
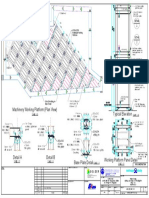
- Reaction Wall: Machinery Working Platform (Plan View) Typical ElevationDocument1 pageReaction Wall: Machinery Working Platform (Plan View) Typical ElevationThi HaNo ratings yet
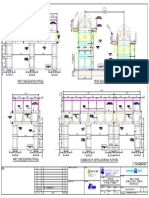
- Part 1 Side Elevation (Typical) Front Elevation (Typical) : GolderDocument1 pagePart 1 Side Elevation (Typical) Front Elevation (Typical) : GolderThi HaNo ratings yet
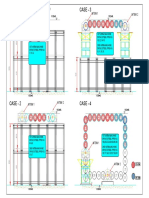
- Case - 1 Case - 3: MTBM 1 MTBM 1 MTBM 2Document1 pageCase - 1 Case - 3: MTBM 1 MTBM 1 MTBM 2Thi HaNo ratings yet
- Contact The ACCC: Who Is Making The Report?Document3 pagesContact The ACCC: Who Is Making The Report?Thi HaNo ratings yet
- Resignation Letter EXCAVATOR OPTRDocument1 pageResignation Letter EXCAVATOR OPTRThi Ha100% (1)
- S/N. Name Position Position S/N. NameDocument1 pageS/N. Name Position Position S/N. NameThi HaNo ratings yet
- Resignation LetterDocument1 pageResignation LetterThi HaNo ratings yet
- Introduction To AluminumDocument33 pagesIntroduction To Aluminumilham fdhlman11No ratings yet
- A Beginner's Guide To Pig FarmingDocument87 pagesA Beginner's Guide To Pig FarmingIdada EzekielNo ratings yet
- The Importance of Earth Loop ImpedanceDocument4 pagesThe Importance of Earth Loop ImpedanceKarim Amer100% (1)
- Meniere's Disease and Tinnitus in Nursing PractiseDocument5 pagesMeniere's Disease and Tinnitus in Nursing PractiseLizbeth MarinahNo ratings yet
- 32 Diet Recipes - Tamil MagazinesDocument11 pages32 Diet Recipes - Tamil MagazinesPandimadevi Selvakumar0% (1)
- Procedures For Analysis of Citrus Products PDFDocument193 pagesProcedures For Analysis of Citrus Products PDFluis100% (2)
- Imogene Martina KingDocument7 pagesImogene Martina KingJoanna Marie TulioNo ratings yet
- 1 - KSU Research Methodology Overview (A Mandil, Oct 2009)Document25 pages1 - KSU Research Methodology Overview (A Mandil, Oct 2009)Fatamii IiiNo ratings yet
- Vocabulary Matching: Paragraph 1Document3 pagesVocabulary Matching: Paragraph 1MarizaNo ratings yet
- Full Floating Clapper Assembly: Swing Check ValveDocument2 pagesFull Floating Clapper Assembly: Swing Check Valvemubarak aliNo ratings yet
- Astm E1973 - 1 (En)Document4 pagesAstm E1973 - 1 (En)Dinesh SaiNo ratings yet
- Jurnal Ilmiah Simantek ISSN. 2550-0414 Vol. 5 No. 1 Februari 2021Document5 pagesJurnal Ilmiah Simantek ISSN. 2550-0414 Vol. 5 No. 1 Februari 2021Muhamad IhsanNo ratings yet
- Technical Bulletin: Ptfe, 25% Glass Filled Slide PlatesDocument5 pagesTechnical Bulletin: Ptfe, 25% Glass Filled Slide PlatesDavid Luna MolinaNo ratings yet
- Appendix 6Document4 pagesAppendix 6Vlad OlariuNo ratings yet
- 310 SRU Thermal Reactor Chemistry and Design SRU Buenos Aires 2018Document27 pages310 SRU Thermal Reactor Chemistry and Design SRU Buenos Aires 2018Nastaran BagheriNo ratings yet
- Benefits of HobbiesDocument6 pagesBenefits of HobbiesAdam YapNo ratings yet
- HB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiDocument23 pagesHB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiMudassar Roomi100% (1)
- Food Fundamentals 10 - E - Margaret McWilliamsDocument497 pagesFood Fundamentals 10 - E - Margaret McWilliamspedropereza88No ratings yet
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- Thuja's Effectiveness Against SmallpoxDocument361 pagesThuja's Effectiveness Against SmallpoxFrank NavaNo ratings yet
- Valtek Beta Positioners: For Control ValvesDocument8 pagesValtek Beta Positioners: For Control Valvesابزار دقیقNo ratings yet
- 15419Document29 pages15419Sadashiva SahooNo ratings yet
- The New Rules To Getting AheadDocument8 pagesThe New Rules To Getting AheadWes LangloisNo ratings yet
- Clear ViewDocument6 pagesClear ViewJamieNo ratings yet
- Ladipur EVA LiquidDocument2 pagesLadipur EVA LiquidKalki VermaNo ratings yet
- Fiat Ducato x250 Natural Power (CNG) Instructions Manual Appendix - ENDocument24 pagesFiat Ducato x250 Natural Power (CNG) Instructions Manual Appendix - ENVhateNo ratings yet
- Data Sheet - BS6231 PVC Tri-Rated Flexible Cable - Cleveland CableDocument2 pagesData Sheet - BS6231 PVC Tri-Rated Flexible Cable - Cleveland CableCalum MartinNo ratings yet
- Smartyou 21 Day PDF PlannerDocument9 pagesSmartyou 21 Day PDF PlannerYarelis Montero Mercado100% (1)
- Ibat-ibang dulog sa paghawak ng klaseDocument2 pagesIbat-ibang dulog sa paghawak ng klaseJovito Limot100% (3)
- Diagrama Electrico 533DDocument2 pagesDiagrama Electrico 533DJordan RaveloNo ratings yet