You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
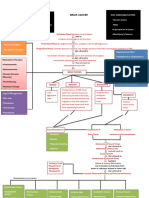
- Brain Cancer Concept MapDocument3 pagesBrain Cancer Concept MapIced Coffee100% (4)
- UFS HACCP Recipe Booklet EnglishDocument20 pagesUFS HACCP Recipe Booklet EnglishAdeyemi Oluwafunminiyi AdeoyeNo ratings yet
- MG - L4 - Mutation & Dna Repair - Part 1Document25 pagesMG - L4 - Mutation & Dna Repair - Part 1Vy KhánhNo ratings yet
- Misconceptions and Safety in Radiation OncologyDocument4 pagesMisconceptions and Safety in Radiation Oncologyapi-633248237No ratings yet
- 2010 STEPS Report BangladeshDocument176 pages2010 STEPS Report Bangladeshfatehatun noorNo ratings yet
- D 5 LRDocument2 pagesD 5 LRDianelie BacenaNo ratings yet
- Child Care What If Child Becomes Sick FlowchartDocument1 pageChild Care What If Child Becomes Sick FlowcharthmareidNo ratings yet
- Biological Psychology Notes - Edexcel (IAL) Psychology A-LevelDocument14 pagesBiological Psychology Notes - Edexcel (IAL) Psychology A-LevelAyse KerimNo ratings yet
- MODULE 6 Sir RobertDocument17 pagesMODULE 6 Sir RobertManilyn DominguezNo ratings yet
- Research Paper: PollutionDocument21 pagesResearch Paper: PollutionJhesbon K CaballesNo ratings yet
- UNIT 11 Zdrowie: Matura - Poziom PodstawowyDocument4 pagesUNIT 11 Zdrowie: Matura - Poziom PodstawowyPaulina MaciszkaNo ratings yet
- At War With Metaphor Media, Propaganda, and Racism... - (Chapter 4)Document30 pagesAt War With Metaphor Media, Propaganda, and Racism... - (Chapter 4)DanNo ratings yet
- Ambien (Zolpidem) Molecule - World of MoleculesDocument8 pagesAmbien (Zolpidem) Molecule - World of MoleculesyunusNo ratings yet
- Overview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateDocument27 pagesOverview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateRopiNo ratings yet
- Care of Unconscious PatientDocument7 pagesCare of Unconscious PatientSallieNo ratings yet
- Sodium BicarbonateDocument8 pagesSodium BicarbonateAljon QuijanoNo ratings yet
- Cystic FibrosisDocument69 pagesCystic FibrosisPadma Sagarika KarriNo ratings yet
- ACLS JeopardyDocument3 pagesACLS JeopardyLaylee Clare100% (1)
- Open Source and Free SoftwareDocument5 pagesOpen Source and Free SoftwareaxlzekeNo ratings yet
- Marketing Management GLDocument11 pagesMarketing Management GLSaravanan VaradharajanNo ratings yet
- What You Should Know Before You Start A Weight-Loss PlanDocument10 pagesWhat You Should Know Before You Start A Weight-Loss PlanRAKESH RANJANNo ratings yet
- Life Intermediate WordlistDocument12 pagesLife Intermediate Wordlistgallipatero33% (3)
- Urethral StrictureDocument35 pagesUrethral StrictureDoctors PodcastNo ratings yet
- Ash LeshaDocument2 pagesAsh Leshaf_factorNo ratings yet
- Statistics: Formula For Rate: AdvantagesDocument3 pagesStatistics: Formula For Rate: AdvantagesJhes D.No ratings yet
- MICROBIOLOGY-4th Year SyllabusDocument13 pagesMICROBIOLOGY-4th Year SyllabusPravesh NiraulaNo ratings yet
- Dias2009 Article PantoprazoleDocument10 pagesDias2009 Article PantoprazoleTan JayNo ratings yet
- Ayurved RitucharyaDocument32 pagesAyurved Ritucharyavasudev gujralNo ratings yet
- Paediatric Clerking SheetDocument5 pagesPaediatric Clerking SheetIamTinesh100% (2)
- Chir 5Document10 pagesChir 5George MogaNo ratings yet