You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (347)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fundamental Molecular Biology: Lisabeth A. AllisonDocument73 pagesFundamental Molecular Biology: Lisabeth A. AllisonJu noNo ratings yet
- 575854100sex-Linked InheritanceDocument18 pages575854100sex-Linked InheritanceMohammad Faizan RazaNo ratings yet
- Martin 1991 - EggSpermDocument9 pagesMartin 1991 - EggSpermBuğu Eylül YAŞARNo ratings yet
- Breeding Plants For Future ClimatesDocument49 pagesBreeding Plants For Future ClimatesFaisal ShehzadNo ratings yet
- Congenital Abnormalities and DysmorphologyDocument5 pagesCongenital Abnormalities and DysmorphologyNaliaka WafulaNo ratings yet
- Puerto Princesa City National Science High SchoolDocument2 pagesPuerto Princesa City National Science High SchoolRodolf Jones RaboNo ratings yet
- M.04 Modes of Inheritance and Pedigree AnalysisDocument4 pagesM.04 Modes of Inheritance and Pedigree Analysisno veNo ratings yet
- Godzilla Vs ZillaDocument4 pagesGodzilla Vs ZillaDaniel McallisterNo ratings yet
- Infographic Folic Acid Vs FolateDocument1 pageInfographic Folic Acid Vs FolateKaterina PoposkaNo ratings yet
- Trichoptera Phylogeny Adaptations and BiogeographyDocument13 pagesTrichoptera Phylogeny Adaptations and BiogeographyCarli RodríguezNo ratings yet
- Chapter 11 - Endocrine SystemDocument13 pagesChapter 11 - Endocrine SystemIvy CustodioNo ratings yet
- 1 - Methods For Biological Examination of FoodsDocument48 pages1 - Methods For Biological Examination of FoodsKim Anh HaNo ratings yet
- RBC ANOMALIES AND INCLUSIONS With Their Associated DiseasesDocument2 pagesRBC ANOMALIES AND INCLUSIONS With Their Associated DiseasesCamella Beatrice Lujan ValleNo ratings yet
- Buenafe JC FoodChem Week 11 To 13Document1 pageBuenafe JC FoodChem Week 11 To 13john buenafeNo ratings yet
- Evolution-History and EvidenceDocument19 pagesEvolution-History and Evidencekatexxx100% (1)
- Polymerase Chain Reaction: Determining The Right Magnesium Chloride Concentration For DNA Amplification of Acetobacter XylinumDocument5 pagesPolymerase Chain Reaction: Determining The Right Magnesium Chloride Concentration For DNA Amplification of Acetobacter XylinumAlyza Joy RamirezNo ratings yet
- Nejmcpc 1102202Document10 pagesNejmcpc 1102202FrinkooFrinkoBNo ratings yet
- HKS123 Introduction To Sports Science Note-1Document32 pagesHKS123 Introduction To Sports Science Note-1ikponmwosavera1No ratings yet
- Postgraduate Handbook 2016 2017Document105 pagesPostgraduate Handbook 2016 2017Aya AmirNo ratings yet
- Effect of ER Stress On Vascular Smooth Muscle CellsDocument95 pagesEffect of ER Stress On Vascular Smooth Muscle CellsaneerajapNo ratings yet
- 21 - 10th Bio Class - 25 Interbell WS - 21 EngDocument3 pages21 - 10th Bio Class - 25 Interbell WS - 21 EngsajithvariathNo ratings yet
- Pener1991, Locust Phase Polymorphism and Its EndocrineDocument79 pagesPener1991, Locust Phase Polymorphism and Its EndocrineAdriano Medeiros de SiqueiraNo ratings yet
- RNA and Protein Synthesis Problem SetDocument6 pagesRNA and Protein Synthesis Problem Setpalms thatshatterNo ratings yet
- MeiosisPuzzle FinalDocument5 pagesMeiosisPuzzle Finalgopan629No ratings yet
- BIO EXP 1 and 2Document7 pagesBIO EXP 1 and 2Bala Murugan.VNo ratings yet
- Position Paper Gen Bio Week 1Document3 pagesPosition Paper Gen Bio Week 1Elle HuangNo ratings yet
- Prolactin BookDocument248 pagesProlactin BookAleksandar KitanovskiNo ratings yet
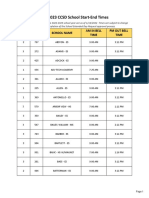
- 2022-2023 CCSD School Start-End TimesDocument23 pages2022-2023 CCSD School Start-End TimesFOX5 Vegas50% (2)
- SIM Biochemistry ULO6Document28 pagesSIM Biochemistry ULO6Darl MalazarteNo ratings yet
- Beckers World of The Cell 9th Edition Hardin Test Bank DownloadDocument23 pagesBeckers World of The Cell 9th Edition Hardin Test Bank Downloaddaddockstudderyxeq100% (28)