You might also like
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (13)
- Medical Certificate FormDocument2 pagesMedical Certificate FormFelipeNo ratings yet
- The Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramFrom EverandThe Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramRating: 5 out of 5 stars5/5 (2)
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- MS Health Claim FormDocument2 pagesMS Health Claim FormBalaji_Rajaman_2280No ratings yet
- Pak Qatar Family Takaful Limited: Hospitalization Reimbursement Claim FormDocument1 pagePak Qatar Family Takaful Limited: Hospitalization Reimbursement Claim Formmastermind_asia9389No ratings yet
- IRDA - Pre Auth FormDocument6 pagesIRDA - Pre Auth FormarunNo ratings yet
- Pre Auth FormDocument2 pagesPre Auth FormRajdeep AdhyaNo ratings yet
- Labor Insurance Maternity Benefit Application Form and Payment Receipt-10806Document2 pagesLabor Insurance Maternity Benefit Application Form and Payment Receipt-10806Krizel Felipe Manglal-lanNo ratings yet
- Pre Auth Form Revised PDFDocument5 pagesPre Auth Form Revised PDFNILESHNo ratings yet
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- Hospital Cash ClaimDocument4 pagesHospital Cash ClaimChloe Auda IbalioNo ratings yet
- CLAIM FORM SUBMISSION GUIDEDocument1 pageCLAIM FORM SUBMISSION GUIDEAnonymous W9VINoTza100% (1)
- FRM GPPF en 0516Document2 pagesFRM GPPF en 0516Adel NewtonNo ratings yet
- New Pre Auth Declaration Form WeAssistDocument4 pagesNew Pre Auth Declaration Form WeAssistSandeep KarkiNo ratings yet
- National Insurance - ClaimFormDocument6 pagesNational Insurance - ClaimFormPallav GangeleNo ratings yet
- National Insurance Company LimitedDocument6 pagesNational Insurance Company LimitedSneha SinhaNo ratings yet
- MD India Insurance Claim FormDocument5 pagesMD India Insurance Claim FormYogesh ParchaniNo ratings yet
- Labor Insurance Maternity Benefit Application Form and Payment ReceiptDocument2 pagesLabor Insurance Maternity Benefit Application Form and Payment ReceiptDeary Ureta PereyraNo ratings yet
- Florida Transfer Guidelines & FormDocument6 pagesFlorida Transfer Guidelines & FormHealth BrookNo ratings yet
- Red Form Labor Insurance Maternity Benefits Application Form - English - LAOBAODocument2 pagesRed Form Labor Insurance Maternity Benefits Application Form - English - LAOBAOBlue DumoneNo ratings yet
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- Ealth Laim Teps: Future Generali HealthDocument3 pagesEalth Laim Teps: Future Generali HealthMarissa DrakeNo ratings yet
- Claim Form Dhs ReimbursementDocument4 pagesClaim Form Dhs ReimbursementrenjithkunnumpurathNo ratings yet
- Medical Insurance Claim Form (Corporate)Document3 pagesMedical Insurance Claim Form (Corporate)hari198902234No ratings yet
- MaxBupa Pre Auth Claim FormDocument5 pagesMaxBupa Pre Auth Claim FormvineetNo ratings yet
- NOW HEALTH Claim - Form - Uae - RsaDocument2 pagesNOW HEALTH Claim - Form - Uae - RsaWilliam IsaacNo ratings yet
- Request for cashless hospitalizationDocument6 pagesRequest for cashless hospitalizationBOOKREADER_NOWNo ratings yet
- Put Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsDocument3 pagesPut Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsTHÍCH XEM XENo ratings yet
- OMA OM en Claims TravelDelayDocument4 pagesOMA OM en Claims TravelDelayreshwan aliNo ratings yet
- Patient Admission FormDocument2 pagesPatient Admission Formelmore kakaNo ratings yet
- Pre Authorisation Form - New CashlessDocument2 pagesPre Authorisation Form - New CashlessMitraNo ratings yet
- Physiomodalities Catlog NewDocument2 pagesPhysiomodalities Catlog NewRKNo ratings yet
- I Health CareDocument1 pageI Health Caredisk_la_poduNo ratings yet
- Claim Form-MD IndiaDocument5 pagesClaim Form-MD IndiaMusycal FynncNo ratings yet
- OPD Claim FormDocument1 pageOPD Claim FormKhalid SayeedNo ratings yet
- Cashless FormDocument2 pagesCashless Formvaisam0% (1)
- FACS ReferralDocument2 pagesFACS Referralsandhupriya1998No ratings yet
- Formular Za Pristanak Na Cijepljenje Na FloridiDocument2 pagesFormular Za Pristanak Na Cijepljenje Na FloridiIndex.hrNo ratings yet
- Medical Report and ReceiptDocument5 pagesMedical Report and Receiptkumarsam087No ratings yet
- Claim Form For Group Personal Accident PoliciesDocument4 pagesClaim Form For Group Personal Accident PoliciesanujaNo ratings yet
- TransferDocument4 pagesTransferDindo NuguidNo ratings yet
- Medical Claim Reimbursement Form EnglishDocument2 pagesMedical Claim Reimbursement Form EnglishHananAhmedNo ratings yet
- Ambulance Billing Frequently Asked Questions: Ems - Customerservice@houstontx - GovDocument5 pagesAmbulance Billing Frequently Asked Questions: Ems - Customerservice@houstontx - GovONo ratings yet
- College CFDocument2 pagesCollege CFPeter IgnacioNo ratings yet
- Chubb14-345-1122 Uber Personal Injury Claim Form-INTDocument7 pagesChubb14-345-1122 Uber Personal Injury Claim Form-INTEidrian RicardoNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument3 pagesHDFC ERGO General Insurance Company LimitedKumar A GovindaNo ratings yet
- Form No: HI / Claim IntimationDocument2 pagesForm No: HI / Claim IntimationVishal SankheNo ratings yet
- Iiisla Benevolent Fund (Ibf) : Claim FormDocument2 pagesIiisla Benevolent Fund (Ibf) : Claim FormSachin PrajapatiNo ratings yet
- Claim Form GeneralDocument1 pageClaim Form GeneralTanya Rose-AppleNo ratings yet
- Admission To HospitalDocument12 pagesAdmission To HospitalM SulistiawanNo ratings yet
- New Claim Form Dhs ReimbursementDocument4 pagesNew Claim Form Dhs Reimbursementamit_bisht2225% (4)
- Parent Consent and Liability Release FormDocument1 pageParent Consent and Liability Release FormVictoria SettleNo ratings yet
- Standard Claim Form InsuredDocument2 pagesStandard Claim Form InsuredknsaravanaNo ratings yet
- Axa Claim FormDocument2 pagesAxa Claim FormReem Mohamed El BarraniNo ratings yet
- BINS Bupa Global Claim Form en 2005 21089Document8 pagesBINS Bupa Global Claim Form en 2005 21089R.Pearlsis SophiNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormElmedina Berin HalilovićNo ratings yet
- Duties and Responsibilities - Pharmacy BusinessDocument4 pagesDuties and Responsibilities - Pharmacy BusinessMA. TRIXIA ANNE KAHULUGANNo ratings yet
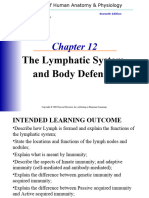
- Lymphatic SystemDocument76 pagesLymphatic SystemChristopher Rey BurceNo ratings yet
- Salbutamol Plus PropranololDocument2 pagesSalbutamol Plus PropranololChristopher Rey BurceNo ratings yet
- Orca Share Media1667471287285 6993881490147826956Document2 pagesOrca Share Media1667471287285 6993881490147826956Christopher Rey BurceNo ratings yet
- A&P Course SyllabusDocument4 pagesA&P Course SyllabusChristopher Rey BurceNo ratings yet
- Triage PPT DownloadDocument15 pagesTriage PPT DownloadEmergency ABMCNo ratings yet
- Design of Sewer SystemDocument8 pagesDesign of Sewer Systemknight912No ratings yet
- Pilot Testing Complex Care CoordinationDocument19 pagesPilot Testing Complex Care CoordinationRavi S GSRNo ratings yet
- Nursing Care of Older PeopleDocument2 pagesNursing Care of Older Peoplehazel gadzikwaNo ratings yet
- IEHP Authorization H2309482488 UM Tran Auth Form ServicingDocument3 pagesIEHP Authorization H2309482488 UM Tran Auth Form ServicingRo DanielaNo ratings yet
- Schmieding Certified Home Caregiver TrainingDocument1 pageSchmieding Certified Home Caregiver Trainingapi-200977699No ratings yet
- Waltham CrossDocument1 pageWaltham CrossKairav HauradhurNo ratings yet
- Mian Shahbaz Sharif Hospital SNEDocument2 pagesMian Shahbaz Sharif Hospital SNEjawad537407No ratings yet
- Sports Rehab Fellowship GuideDocument6 pagesSports Rehab Fellowship Guidesendilcoumarv83No ratings yet
- Good-Pharmacy-Practice Certificate of Achievement DvyjlbbDocument2 pagesGood-Pharmacy-Practice Certificate of Achievement Dvyjlbbparwana formuliNo ratings yet
- Current CDTA System Map (Winter 2011)Document1 pageCurrent CDTA System Map (Winter 2011)Andy ArthurNo ratings yet
- Abbreviations used in result headingsDocument17 pagesAbbreviations used in result headingsSachin IngoleNo ratings yet
- ExpandedroleofnursesDocument17 pagesExpandedroleofnursesRaquel M. MendozaNo ratings yet
- Bondi Junction Network Map: LegendDocument3 pagesBondi Junction Network Map: LegendRichie ValladaresNo ratings yet
- NCM103 - Chapter Test PDFDocument4 pagesNCM103 - Chapter Test PDFFrancine Dominique CollantesNo ratings yet
- Consultation Liaison PsychiatryDocument25 pagesConsultation Liaison Psychiatrybintag mahaputraNo ratings yet
- Route71 ScheduleDocument1 pageRoute71 ScheduleQinrun GeNo ratings yet
- Postal Manual Volume VDocument187 pagesPostal Manual Volume VLatest Laws Team100% (2)
- Outscraper-20240212072502e047 Pharmaceutical Products Wholesaler +2Document84 pagesOutscraper-20240212072502e047 Pharmaceutical Products Wholesaler +2sanjulata.agriNo ratings yet
- PLDT Area CodesDocument53 pagesPLDT Area Codesjosh0% (1)
- 2 WEBSITE RA-NURSE - Baguio - 5-2023Document73 pages2 WEBSITE RA-NURSE - Baguio - 5-2023kazel DantesNo ratings yet
- Phos 313 - Activity No 7 PhosDocument6 pagesPhos 313 - Activity No 7 PhosDIANA CAMILLE CARITATIVONo ratings yet
- NicoyDocument3 pagesNicoyHanz AndreiNo ratings yet
- Comparative Study BetweenDocument15 pagesComparative Study BetweenAfzal PetiwalaNo ratings yet
- Ethics AssignmentDocument3 pagesEthics AssignmentNia OliverNo ratings yet
- My CPPE BookingsDocument1 pageMy CPPE BookingsMohamed HamirNo ratings yet
- Amina 2Document2 pagesAmina 2Aliyu TanimuNo ratings yet
- E-Prescribing by ShamaDocument1 pageE-Prescribing by ShamaAnika Tabassum ShamaNo ratings yet
- Date Sheet For The Doctor of Pharmacy PharmD Annual Examination 2023 t8008Document2 pagesDate Sheet For The Doctor of Pharmacy PharmD Annual Examination 2023 t8008Haniya RajpootNo ratings yet
- Mobility Management and Public Infrastructure InnovationDocument45 pagesMobility Management and Public Infrastructure InnovationAngeli MarzanNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)