You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- F.E. Campbell - Sweet Slavery - HIT 139Document115 pagesF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 01 Well Head ComponentsDocument46 pages01 Well Head ComponentsKhanh Pham Minh100% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Logiqids Sample Paper KG FinalDocument15 pagesLogiqids Sample Paper KG FinalShenbaga Devi PadmanabanNo ratings yet
- Business Plan Hair DyeDocument12 pagesBusiness Plan Hair Dyercool_rahul0039341No ratings yet
- WCDMA Optimization Case StudyDocument60 pagesWCDMA Optimization Case StudyRamesh Nikam100% (1)
- Torc 4 Abscohort1 - CompressDocument13 pagesTorc 4 Abscohort1 - CompressFaye MartinezNo ratings yet
- Soal Tes TOEFL Dan Pembahasan Jawaban StructureDocument48 pagesSoal Tes TOEFL Dan Pembahasan Jawaban Structureemi agus triani88% (51)
- GORUCK Heavy - 6-week training program overviewDocument4 pagesGORUCK Heavy - 6-week training program overviewJohn Rohrer100% (2)
- Music and Therapy Bun2Document17 pagesMusic and Therapy Bun2PanteaAlisaNo ratings yet
- STM - Merck Case AnswersDocument2 pagesSTM - Merck Case AnswersreetayanNo ratings yet
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- Nutrición Hospitalaria 0212-1611: IssnDocument7 pagesNutrición Hospitalaria 0212-1611: IssnelenaNo ratings yet
- Curs 12Document30 pagesCurs 12mariana maricelaNo ratings yet
- Australian Dental JournalDocument7 pagesAustralian Dental JournalelenaNo ratings yet
- Buletin LP 1Document5 pagesBuletin LP 1Georgiana RosulescuNo ratings yet
- Alfonso Rosa2013Document7 pagesAlfonso Rosa2013elenaNo ratings yet
- SEO-Optimized Title for Medical Synonyms ListDocument11 pagesSEO-Optimized Title for Medical Synonyms ListDan Stefan AninoiuNo ratings yet
- Loss of Olfactory Function and Nutritional Status in Vital Older Adults and Geriatric PatientsDocument7 pagesLoss of Olfactory Function and Nutritional Status in Vital Older Adults and Geriatric PatientselenaNo ratings yet
- Influence of Nutritional Status On Health-Related Quality of Life of Non-Institutionalized Older PeopleDocument6 pagesInfluence of Nutritional Status On Health-Related Quality of Life of Non-Institutionalized Older PeopleelenaNo ratings yet
- F PO 7.5.1 03 Test Partial 2Document4 pagesF PO 7.5.1 03 Test Partial 2elenaNo ratings yet
- TOEFL VocaDocument46 pagesTOEFL Vocaibov100% (9)
- VMware Log File Shows System StartupDocument1,180 pagesVMware Log File Shows System StartupelenaNo ratings yet
- Programa in Engleza A1Document11 pagesPrograma in Engleza A1elenaNo ratings yet
- Cuvinte Limba Engleza-Medicina GeneralaDocument4 pagesCuvinte Limba Engleza-Medicina GeneralaRait von Jakhia100% (4)
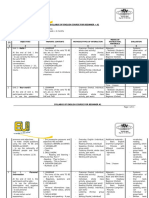
- The English Syllabus for Pre-Intermediate Level B1Document21 pagesThe English Syllabus for Pre-Intermediate Level B1elenaNo ratings yet
- Programa in Engleza A2Document18 pagesPrograma in Engleza A2elena100% (1)
- Stop and Check 3: I. Underline The Correct Verb FormDocument3 pagesStop and Check 3: I. Underline The Correct Verb FormelenaNo ratings yet
- Harap Alb PDFDocument17 pagesHarap Alb PDFelenaNo ratings yet
- Acestea 3 Sunt Dictionarele Pe Care Le Utilizez Eu in Mod FrecventDocument1 pageAcestea 3 Sunt Dictionarele Pe Care Le Utilizez Eu in Mod FrecventelenaNo ratings yet
- F-PO-7.5.1-04 Test Final A1Document3 pagesF-PO-7.5.1-04 Test Final A1elenaNo ratings yet
- Manual Biologie Clasa XI - A, Editura Corint PDFDocument129 pagesManual Biologie Clasa XI - A, Editura Corint PDFDuluman Razvan100% (1)
- Harap Alb PDFDocument17 pagesHarap Alb PDFelenaNo ratings yet
- In Gradina GDocument2 pagesIn Gradina GelenaNo ratings yet
- Suhana Pravin Masale & PicklesDocument11 pagesSuhana Pravin Masale & PicklesSijo Kunjumon100% (1)
- Acp 22 9349 2022Document20 pagesAcp 22 9349 2022merlinakisNo ratings yet
- Holy Childhood High School Chemistry 601 Topic: Electronic StructureDocument6 pagesHoly Childhood High School Chemistry 601 Topic: Electronic StructureBriana BartonNo ratings yet
- Economic Case for Immobilizing EnzymesDocument25 pagesEconomic Case for Immobilizing EnzymesNikki ChauhanNo ratings yet
- W H G Kingston "Dick Cheveley": PrefaceDocument159 pagesW H G Kingston "Dick Cheveley": PrefaceGutenberg.orgNo ratings yet
- Wheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesDocument9 pagesWheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesmaurodiloretoNo ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- Ni 2 WordDocument2 pagesNi 2 WordLeigh Angelika Dela CruzNo ratings yet
- Pensions Reforms at NSSFDocument4 pagesPensions Reforms at NSSFcliffmogere2348No ratings yet
- Flashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelDocument37 pagesFlashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelTravel UnlimitedNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Preparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionDocument12 pagesPreparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionPaula NancyNo ratings yet
- Strengthening HIV Care in Africa CertificateDocument7 pagesStrengthening HIV Care in Africa CertificateMaiga Ayub HusseinNo ratings yet
- What Are OPPE and FPPE?Document1 pageWhat Are OPPE and FPPE?adyNo ratings yet
- Effect of Non-Newtonian Fluids On The Performance of Plate Type Heat ExchangerDocument4 pagesEffect of Non-Newtonian Fluids On The Performance of Plate Type Heat Exchangerdeepika snehiNo ratings yet
- Menu Baru Kopi GandapoeraDocument7 pagesMenu Baru Kopi GandapoeraAlwan AhpNo ratings yet
- Amul India Case Study: Product Portfolio and SWOT AnalysisDocument10 pagesAmul India Case Study: Product Portfolio and SWOT AnalysisShruti NagmoteNo ratings yet
- Deliver VALUE and RENEWABLE FUTUREDocument30 pagesDeliver VALUE and RENEWABLE FUTUREAlexandru SuciuNo ratings yet
- SP-200 Advanced PumpDocument4 pagesSP-200 Advanced PumpOsvaldo BravoNo ratings yet