You might also like
- Neonatal Nursing: Scope and Standards of PracticeFrom EverandNeonatal Nursing: Scope and Standards of PracticeRating: 4 out of 5 stars4/5 (1)
- BNCresusDocument21 pagesBNCresusBagas Praditya putraNo ratings yet
- Antenatal CareDocument7 pagesAntenatal CareMUBARAK HUSSAININo ratings yet
- Nursing the NeonateFrom EverandNursing the NeonateMaggie MeeksNo ratings yet
- Essential Newborn Care Practices and Associated Factors Among Home Delivered Mothers in Damot Pulasa Woreda, Southern EthiopiaDocument11 pagesEssential Newborn Care Practices and Associated Factors Among Home Delivered Mothers in Damot Pulasa Woreda, Southern EthiopiaalchmistNo ratings yet
- An Analysis of Impact of Antenatl Care in Reducing Maternal Mortality RateDocument46 pagesAn Analysis of Impact of Antenatl Care in Reducing Maternal Mortality RateUsman Ahmad TijjaniNo ratings yet
- Bemoc GuideDocument193 pagesBemoc GuideCindy Rose MisenaNo ratings yet
- Antenatal and Postnatal CareDocument12 pagesAntenatal and Postnatal CarehiwaNo ratings yet
- Introduction To QoC SurveysDocument8 pagesIntroduction To QoC SurveysBaleegh Al-sharabyNo ratings yet
- Ijwh 7 239Document4 pagesIjwh 7 239Wahyu WeraNo ratings yet
- The Nature of Scholarship, a Career Legacy Map and Advanced Practice: An Important TriadFrom EverandThe Nature of Scholarship, a Career Legacy Map and Advanced Practice: An Important TriadNo ratings yet
- Midwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaDocument11 pagesMidwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaAdhiw AmanNo ratings yet
- National Guidelines For Quality Obstetrics and Perinatal Care PDFDocument410 pagesNational Guidelines For Quality Obstetrics and Perinatal Care PDFduncan100% (1)
- Factors Affecting Utilization of Antenatal Care in Ethiopia: A Systematic Review and Meta-AnalysisDocument24 pagesFactors Affecting Utilization of Antenatal Care in Ethiopia: A Systematic Review and Meta-AnalysisWidhia Tyas WentNo ratings yet
- Quality of Care For Pregnant Women and Newborns - The WHO VisionDocument5 pagesQuality of Care For Pregnant Women and Newborns - The WHO Visionrestu pangestutiNo ratings yet
- Evidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsDocument15 pagesEvidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsLore Anne Mhae SantosNo ratings yet
- Pengalaman Tenaga Kesehatan Menangani Fetal DistresDocument11 pagesPengalaman Tenaga Kesehatan Menangani Fetal DistresAtikah AbayNo ratings yet
- Awareness of The Impact of Ante-Natal Care (Anc) Services in PreventingDocument8 pagesAwareness of The Impact of Ante-Natal Care (Anc) Services in PreventingUsman Ahmad TijjaniNo ratings yet
- Antenatal CareDocument12 pagesAntenatal CarefiramnNo ratings yet
- IMPAC Tool for Making Pregnancy SaferDocument16 pagesIMPAC Tool for Making Pregnancy SaferLea Foy-os CapiliNo ratings yet
- Predictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDocument8 pagesPredictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDessy WahyuniNo ratings yet
- EngDocument54 pagesEngAiralyn Chavez Alaro100% (1)
- Utilization of Antenatal Care Services by Urban Squatters of Kathmandu ValleyDocument6 pagesUtilization of Antenatal Care Services by Urban Squatters of Kathmandu ValleyPramila PoudelNo ratings yet
- retrospective cohrt3Document10 pagesretrospective cohrt3Degefa HelamoNo ratings yet
- Implications of the IOM's Future of Nursing ReportDocument8 pagesImplications of the IOM's Future of Nursing Reportعبدالمحسن علي ENo ratings yet
- Essential Components of Postnatal Care - A Systematic Literature Review and Development of Signal Functions To Guide Monitoring and EvaluationDocument16 pagesEssential Components of Postnatal Care - A Systematic Literature Review and Development of Signal Functions To Guide Monitoring and EvaluationvineelainjetyNo ratings yet
- A Handbook for Student Nurses, second edition: Introducing Key Issues Relevant for PracticeFrom EverandA Handbook for Student Nurses, second edition: Introducing Key Issues Relevant for PracticeNo ratings yet
- ICNP Catalogue Prenatal Nursing CareDocument24 pagesICNP Catalogue Prenatal Nursing CareMitz BaldizarNo ratings yet
- Tun-Alp Et al-2017-BJOG ANCguidelinecommentaryDocument3 pagesTun-Alp Et al-2017-BJOG ANCguidelinecommentaryFitria NurwulansariNo ratings yet
- Pre Eclampsia ManualDocument48 pagesPre Eclampsia ManualFilipa Pimenta de MatosNo ratings yet
- HEAT LDC Final Print Output Cropped 20 PDFDocument170 pagesHEAT LDC Final Print Output Cropped 20 PDFbaasheNo ratings yet
- Who PCPNC PDFDocument179 pagesWho PCPNC PDFTiffany Joyce MarcellanaNo ratings yet
- Skilled Birth Attendance-Lessons LearntDocument9 pagesSkilled Birth Attendance-Lessons LearntTriksha GeorgeNo ratings yet
- Newborn Care Until The First Week of LifeDocument66 pagesNewborn Care Until The First Week of LifeJan Audan100% (1)
- Business DevelopemntDocument17 pagesBusiness Developemntayan ghoshNo ratings yet
- Operational Guidelines For Establishing Sentinel Stillbirth Surveillance SystemDocument40 pagesOperational Guidelines For Establishing Sentinel Stillbirth Surveillance Systemraval anil.uNo ratings yet
- Maternal and Newborn Health ProtocolDocument172 pagesMaternal and Newborn Health ProtocolTheophilus BaidooNo ratings yet
- COIN.2017 Participants ManualDocument106 pagesCOIN.2017 Participants ManualTalent GraysonNo ratings yet
- Quality of Postnatal Care ServicesDocument10 pagesQuality of Postnatal Care Servicessaleha sultanaNo ratings yet
- PPHmanagement DrBenedictDocument17 pagesPPHmanagement DrBenedictPriyanka Vikas TakNo ratings yet
- Post Natal Care Etiopia PDFDocument108 pagesPost Natal Care Etiopia PDFmedicina tradicionalNo ratings yet
- 8 CounteverynewbornDocument24 pages8 CounteverynewbornFitriNo ratings yet
- Improving Health Literacy Through Group Antenatal CareDocument9 pagesImproving Health Literacy Through Group Antenatal Carenuno ferreiraNo ratings yet
- Preconception Care To Improve Pregnancy Outcomes: The ScienceDocument8 pagesPreconception Care To Improve Pregnancy Outcomes: The SciencekofiNo ratings yet
- Healthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009From EverandHealthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009No ratings yet
- Indicators Towards Monitoring Progress Towards Maternal and Newborn Survival RevisedDocument5 pagesIndicators Towards Monitoring Progress Towards Maternal and Newborn Survival RevisedJobelle Fernandez-SantosNo ratings yet
- 1Document11 pages1PSIK sarimuliaNo ratings yet
- Induction of Labour: April 2022Document23 pagesInduction of Labour: April 2022Ahmad NazharNo ratings yet
- ARTICULO7Document14 pagesARTICULO7VivisnNo ratings yet
- Bab 1 Bu HanikDocument39 pagesBab 1 Bu HanikYohanes DokaNo ratings yet
- Cfhi ManualDocument160 pagesCfhi Manualapi-246003035No ratings yet
- Antenatal Care BJOGDocument3 pagesAntenatal Care BJOGBusyra HanimNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument10 pagesJurnal Kedokteran Dan Kesehatan IndonesiaAmelia MeilaniNo ratings yet
- Outbreaks, Epidemics, and Health Security: COVID-19 and Ensuring Future Pandemic Preparedness in Ireland and the WorldFrom EverandOutbreaks, Epidemics, and Health Security: COVID-19 and Ensuring Future Pandemic Preparedness in Ireland and the WorldNo ratings yet
- A Critical Look at Exclusive Breastfeeding in Af 2021 International JournalDocument9 pagesA Critical Look at Exclusive Breastfeeding in Af 2021 International JournalRonald QuezadaNo ratings yet
- Training improves emergency obstetric careDocument14 pagesTraining improves emergency obstetric carePratikaLawrenceSasubeNo ratings yet
- Yerophc Final ModelDocument1 pageYerophc Final ModelAr. Libin K BabyNo ratings yet
- YERPHC FINAL (2) - ModelDocument1 pageYERPHC FINAL (2) - ModelAr. Libin K BabyNo ratings yet
- Q1 - Q5 Carry One Mark Each.: GA - General AptitudeDocument26 pagesQ1 - Q5 Carry One Mark Each.: GA - General AptitudeAr. Libin K BabyNo ratings yet
- Yerphc Final (1) - ModelDocument1 pageYerphc Final (1) - ModelAr. Libin K BabyNo ratings yet
- YERR FINAL-Model - PDF 1Document1 pageYERR FINAL-Model - PDF 1Ar. Libin K BabyNo ratings yet
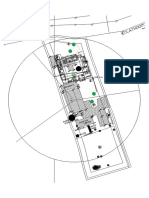
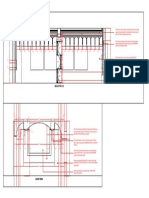
- Yeroor PHC Final (1) - ModelDocument1 pageYeroor PHC Final (1) - ModelAr. Libin K BabyNo ratings yet
- Facade Branding For Health & Wellness Centres: Reference ManualDocument84 pagesFacade Branding For Health & Wellness Centres: Reference ManualTilak ReddyNo ratings yet
- Humanitarian ArchitectureDocument265 pagesHumanitarian ArchitectureRula Rtf100% (2)
- Activity Plan: Project - Health Care Delivery in AnchalDocument1 pageActivity Plan: Project - Health Care Delivery in AnchalAr. Libin K BabyNo ratings yet
- AR Architecture and Planning: Part A: GeneralDocument2 pagesAR Architecture and Planning: Part A: Generalmayur patilNo ratings yet
- Security Combined PDFDocument3 pagesSecurity Combined PDFAr. Libin K BabyNo ratings yet
- AR Architecture and Planning: Part A: GeneralDocument2 pagesAR Architecture and Planning: Part A: Generalmayur patilNo ratings yet
- Premium Satin Enamel for Wood, Wall & MetalDocument6 pagesPremium Satin Enamel for Wood, Wall & MetalAr. Libin K BabyNo ratings yet
- Apcolite Premium Gloss Enamel PDFDocument2 pagesApcolite Premium Gloss Enamel PDFAnand Chavan Projects-QualityNo ratings yet
- GI ID5 Va.0 OFFICE LKB-ELEVATIONSDocument1 pageGI ID5 Va.0 OFFICE LKB-ELEVATIONSAr. Libin K BabyNo ratings yet
- GI - ID5 - Va.0 - OFFICE - LKB-REFLECTED CEILING PLANDocument1 pageGI - ID5 - Va.0 - OFFICE - LKB-REFLECTED CEILING PLANAr. Libin K BabyNo ratings yet
- Interior Works at Gambier International Pvt. LTD.: False CeilingDocument1 pageInterior Works at Gambier International Pvt. LTD.: False CeilingAr. Libin K BabyNo ratings yet
- Boq For Interior WorksDocument1 pageBoq For Interior WorksAr. Libin K BabyNo ratings yet
- Decorative Ceiling Design SpecificationsDocument1 pageDecorative Ceiling Design SpecificationsAr. Libin K BabyNo ratings yet
- GI - ID5 - Va.0 - OFFICE - LKB-KEY PLANDocument1 pageGI - ID5 - Va.0 - OFFICE - LKB-KEY PLANAr. Libin K BabyNo ratings yet
- Office Layout12Document1 pageOffice Layout12Ar. Libin K BabyNo ratings yet
- Plan Section: 12mm Plywood With Laminate Finish TURQUOISE TEAK 5344 GreenlamDocument1 pagePlan Section: 12mm Plywood With Laminate Finish TURQUOISE TEAK 5344 GreenlamAr. Libin K BabyNo ratings yet
- Indian Public Health Standards (IPHS) For Sub-Centres: DraftDocument60 pagesIndian Public Health Standards (IPHS) For Sub-Centres: DraftRekha ChakrabartiNo ratings yet
- Baseline Assessment of Primary Healthcare Delivery Through Subcenters of Northern IndiaDocument12 pagesBaseline Assessment of Primary Healthcare Delivery Through Subcenters of Northern IndiaAr. Libin K BabyNo ratings yet
- German Management & Services v. CA, G.R. No. l-76216 September 14, 1989Document3 pagesGerman Management & Services v. CA, G.R. No. l-76216 September 14, 1989brahmsNo ratings yet
- States' Rights and Global Governance ChallengesDocument2 pagesStates' Rights and Global Governance ChallengesRuby ArcigaNo ratings yet
- WikiLeaks Site Leaks Secret DocumentsDocument48 pagesWikiLeaks Site Leaks Secret DocumentsCh Muhammad ShahidNo ratings yet
- Bus. Org. I Cases Dispute Over Family CorporationDocument166 pagesBus. Org. I Cases Dispute Over Family CorporationBANanaispleetNo ratings yet
- Rosete vs. LimDocument4 pagesRosete vs. LimLoren MandaNo ratings yet
- WC Ritchie V.wayman 244 Ill. 509, 91 N.E. 695Document11 pagesWC Ritchie V.wayman 244 Ill. 509, 91 N.E. 695Thalia SandersNo ratings yet
- Tutorial Exercise Pad 102Document9 pagesTutorial Exercise Pad 102Zian Douglas100% (1)
- Successful Wildlife Crime Prosecution in EuropeDocument9 pagesSuccessful Wildlife Crime Prosecution in EuropeEmilian DrancaNo ratings yet
- September 2020Document92 pagesSeptember 2020Pulkit VashishthNo ratings yet
- MC Facebook CaseDocument4 pagesMC Facebook CaseNamanNo ratings yet
- 1991 S C M R 209 Services MatterDocument5 pages1991 S C M R 209 Services Matterkhaldi askNo ratings yet
- Ra 9282Document6 pagesRa 9282Glen VillanuevaNo ratings yet
- Raghvendra Singh Tomar Vs ED MPHC - 21-Feb-2023 - DigiDocument7 pagesRaghvendra Singh Tomar Vs ED MPHC - 21-Feb-2023 - DigiSandeep DashNo ratings yet
- File Federal Suit in 3 StepsDocument6 pagesFile Federal Suit in 3 StepsTiger Dimension-El100% (5)
- 11 - 2 - 2013 IR Pt. 14082013Document4 pages11 - 2 - 2013 IR Pt. 14082013Vigneshwar Raju PrathikantamNo ratings yet
- Bautista V. Castro Digest By: Shekinah Mae Fortuna FactsDocument1 pageBautista V. Castro Digest By: Shekinah Mae Fortuna FactsShimi FortunaNo ratings yet
- DNR 2018-Final WebDocument144 pagesDNR 2018-Final WebAristegui Noticias100% (1)
- Department of Labor: AppealsDocument6 pagesDepartment of Labor: AppealsUSA_DepartmentOfLabor100% (1)
- Bengzon V Senate Blue Ribbon CommitteeDocument2 pagesBengzon V Senate Blue Ribbon CommitteeKarlyn Ann MagulimanNo ratings yet
- Ha Huynh Columbia Southern University BUS 6320 Global Strategic Management Dr. Michael Morris October 12, 2021Document3 pagesHa Huynh Columbia Southern University BUS 6320 Global Strategic Management Dr. Michael Morris October 12, 2021Hạnh NguyễnNo ratings yet
- Defamation Law BasicsDocument50 pagesDefamation Law BasicsKartik GuptaNo ratings yet
- People v. Salvilla, G.R. No. 86163, April 26, 1990Document12 pagesPeople v. Salvilla, G.R. No. 86163, April 26, 1990Kriszan ManiponNo ratings yet
- Will Privatization Do Any Good To IndiaDocument9 pagesWill Privatization Do Any Good To IndiasumanNo ratings yet
- Bola VoliDocument123 pagesBola Voliina mujiyanaNo ratings yet
- US Vs CaballeroDocument1 pageUS Vs CaballeroGladys BantilanNo ratings yet
- PRESENTATION: The HIV Prevention in Big Cities ProjectDocument7 pagesPRESENTATION: The HIV Prevention in Big Cities ProjectADB Health Sector GroupNo ratings yet
- 1.3 - 1.4 Understand Legal and Regulatory Issues That Pertain To Information Security in A GlobalDocument29 pages1.3 - 1.4 Understand Legal and Regulatory Issues That Pertain To Information Security in A GlobalManoj SharmaNo ratings yet
- Antz CritiqueDocument5 pagesAntz CritiqueJazzel ManaloNo ratings yet
- Central Excise Act 1944Document5 pagesCentral Excise Act 1944lnaveenkNo ratings yet
- 10 Social Science Pol Revision Notes ch4Document4 pages10 Social Science Pol Revision Notes ch4mustansir rangwalaNo ratings yet