You might also like
- LWUA Operation and Maintenance ManualDocument433 pagesLWUA Operation and Maintenance ManualSarahGarcia86% (7)
- Path CNS Robbins Outline: Owl Club Review Sheets 1Document37 pagesPath CNS Robbins Outline: Owl Club Review Sheets 1Coy NuñezNo ratings yet
- Behavioural Pediatrics and Pediatric NursingDocument21 pagesBehavioural Pediatrics and Pediatric Nursingraji100% (7)
- Herling Et Al-2018-Cochrane Database of Systematic ReviewsDocument104 pagesHerling Et Al-2018-Cochrane Database of Systematic ReviewsRodrigoSachiFreitasNo ratings yet
- Needle Aspiration Versus Intercostal Tube Drainage For Pneumothorax ReviewDocument28 pagesNeedle Aspiration Versus Intercostal Tube Drainage For Pneumothorax ReviewFajar YuniftiadiNo ratings yet
- Cochrane Database of Systematic Reviews (Reviews) - Hing, Caroline B - 2011Document45 pagesCochrane Database of Systematic Reviews (Reviews) - Hing, Caroline B - 2011lite.trawler-0xNo ratings yet
- Cochrane Systematic ReviewDocument29 pagesCochrane Systematic ReviewSantiago Sandoval JiménezNo ratings yet
- CD005259 PDFDocument20 pagesCD005259 PDFSandy CuevaNo ratings yet
- Occlusal Adjustment For Treating and Preventing Temporomandibular Joint Disorders ReviewDocument25 pagesOcclusal Adjustment For Treating and Preventing Temporomandibular Joint Disorders ReviewMostafa HassanNo ratings yet
- Gibson Et Al 2017Document65 pagesGibson Et Al 2017marcelo mhNo ratings yet
- Interventions For Dissociated Vertical Deviation (Review) : CochraneDocument37 pagesInterventions For Dissociated Vertical Deviation (Review) : CochraneMacarena AlvarezNo ratings yet
- Lateral PositionDocument162 pagesLateral PositionParli HarunNo ratings yet
- Cambios Estilo de Vida GOTADocument33 pagesCambios Estilo de Vida GOTAMarcela Catalina Fandiño VargasNo ratings yet
- Antibiotic Prophylaxis For Preventing Meningitis in Patients With Basilar Skull Fractures (Review)Document33 pagesAntibiotic Prophylaxis For Preventing Meningitis in Patients With Basilar Skull Fractures (Review)Akmal Niam FirdausiNo ratings yet
- Enthoven 2016Document71 pagesEnthoven 2016Elizabeth VivancoNo ratings yet
- Dafpus SGB 20Document32 pagesDafpus SGB 20Anggie Pradetya MaharaniNo ratings yet
- Acetyl Cholinesterase Inhibitor Treatment For Myasthenia Review (Wiley)Document20 pagesAcetyl Cholinesterase Inhibitor Treatment For Myasthenia Review (Wiley)dewiprahazNo ratings yet
- Vascular Dementia and AcupunctureDocument19 pagesVascular Dementia and AcupunctureMac Gerald CuetoNo ratings yet
- Wang - 2017Document52 pagesWang - 2017Daniel FilizzolaNo ratings yet
- Extracorporeal Shock Wave Therapy For The Healing and Management of Venous Leg UlcersDocument22 pagesExtracorporeal Shock Wave Therapy For The Healing and Management of Venous Leg UlcersAdriana GonzalezNo ratings yet
- Spinal Immobilisation or TraumaDocument20 pagesSpinal Immobilisation or Traumaeli romeroNo ratings yet
- Mathai Et Al-2013-Cochrane Database of Systematic ReviewsDocument38 pagesMathai Et Al-2013-Cochrane Database of Systematic ReviewsBea SphNo ratings yet
- West (2005) - Interventions For Apraxia of Speech Following Stroke)Document14 pagesWest (2005) - Interventions For Apraxia of Speech Following Stroke)ConnieSwiftNo ratings yet
- Stapled Versus Handsewn Methods For Colorectal Anastomosis Surgery (Review)Document53 pagesStapled Versus Handsewn Methods For Colorectal Anastomosis Surgery (Review)Andres Felipe ArizaNo ratings yet
- Tapentadol For Chronic Musculoskeletal Pain in Adults (Review)Document35 pagesTapentadol For Chronic Musculoskeletal Pain in Adults (Review)some buddyyNo ratings yet
- Cochrane Review 2015Document32 pagesCochrane Review 2015Eirini VassilakiNo ratings yet
- Early Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsDocument25 pagesEarly Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsagusNo ratings yet
- Acupuncture For Dysphagia in Acute Stroke (Review) : Xie Y, Wang L, He J, Wu TDocument23 pagesAcupuncture For Dysphagia in Acute Stroke (Review) : Xie Y, Wang L, He J, Wu TegekeskinNo ratings yet
- AVC - Revisao ReabDocument134 pagesAVC - Revisao ReabLuis SeixasNo ratings yet
- Non-Pharmacological Interventions For Chronic Pain in Multiple SclerosisDocument59 pagesNon-Pharmacological Interventions For Chronic Pain in Multiple SclerosisJoana ValenteNo ratings yet
- Deorange2017 PDFDocument51 pagesDeorange2017 PDFMaría Paula Sarmiento RamónNo ratings yet
- Treatment For Ulnar Neuropathy at The Elbow (Review) - Cochrane Database of Systematic Reviews - Caliandro Et Al. - 2016Document47 pagesTreatment For Ulnar Neuropathy at The Elbow (Review) - Cochrane Database of Systematic Reviews - Caliandro Et Al. - 2016Rafaela BatistaNo ratings yet
- Tens Chronic Pain 2010Document62 pagesTens Chronic Pain 2010nandhini raguNo ratings yet
- Antibióticos para La Neumonía Asociada Al Ventilador.Document96 pagesAntibióticos para La Neumonía Asociada Al Ventilador.Julio GonzalesNo ratings yet
- Sharif Et Al-2010-The Cochrane LibraryDocument16 pagesSharif Et Al-2010-The Cochrane LibraryMorohai DoinaNo ratings yet
- Oral Hygiene in VentilatorDocument136 pagesOral Hygiene in VentilatorFelicia Risca RyandiniNo ratings yet
- 2016 - Stem Cell Therapy For Chronic Ischaemic Heart Disease and Congestive HFDocument122 pages2016 - Stem Cell Therapy For Chronic Ischaemic Heart Disease and Congestive HFNicoleta Popa-FoteaNo ratings yet
- Brown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Document44 pagesBrown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Iqra AnugerahNo ratings yet
- Chochrane LibraryDocument83 pagesChochrane LibrarynorizaNo ratings yet
- Chang 1996Document41 pagesChang 1996Miguel Angel Ruiz MarquezNo ratings yet
- 2017 Petunjuk Bayar RegDocument24 pages2017 Petunjuk Bayar RegFrits Dede SinagaNo ratings yet
- Romano Et Al-2012Document34 pagesRomano Et Al-2012ErnestoNo ratings yet
- Wasiak Et Al-2014-The Cochrane LibraryDocument21 pagesWasiak Et Al-2014-The Cochrane LibrarydsNo ratings yet
- Abscesos Drenaje y Fistula CochraneDocument17 pagesAbscesos Drenaje y Fistula CochraneAgustina ZabiniNo ratings yet
- Vasopressors For ShockDocument21 pagesVasopressors For ShocknugrahaNo ratings yet
- Physical Interventions To Interrupt The Spread of Respiratory Viruses - CopyrightedDocument85 pagesPhysical Interventions To Interrupt The Spread of Respiratory Viruses - CopyrightedShirley Pigott MDNo ratings yet
- Snoezelen For DementiaDocument25 pagesSnoezelen For Dementiacati.santiago.castNo ratings yet
- Efficacy and Safety of Cesarean Delivery For Prevention of Mother-To-Child Transmission of HIV-1 (Review)Document15 pagesEfficacy and Safety of Cesarean Delivery For Prevention of Mother-To-Child Transmission of HIV-1 (Review)Herry SasukeNo ratings yet
- Acute Laryngitis in Adult PDFDocument27 pagesAcute Laryngitis in Adult PDFaveNo ratings yet
- Physical Activity and Exercise For Chronic Pain in AdultsDocument77 pagesPhysical Activity and Exercise For Chronic Pain in AdultsgabhekNo ratings yet
- Non Stereoidal Anti Inflammatory Drugs For Chronic Non Cancer Pain in Children and AdolescentsDocument65 pagesNon Stereoidal Anti Inflammatory Drugs For Chronic Non Cancer Pain in Children and AdolescentsMai PyonNo ratings yet
- Antibiotics For Preventing Infection in Open Limb Fractures (Review)Document29 pagesAntibiotics For Preventing Infection in Open Limb Fractures (Review)Krado CroozNo ratings yet
- Buch Binder 2003Document48 pagesBuch Binder 2003Azmi FarhadiNo ratings yet
- Cochrane Database of Systematic ReviewsInterventions For Congenital Talipes EquinovarusDocument65 pagesCochrane Database of Systematic ReviewsInterventions For Congenital Talipes EquinovarusadynataciayadiNo ratings yet
- SA Balneo Vs ExoDocument47 pagesSA Balneo Vs ExoCiana DeseigneNo ratings yet
- Probiotics For People With Hepatic Encephalopathy (Review) : CochraneDocument112 pagesProbiotics For People With Hepatic Encephalopathy (Review) : Cochraneralu_marysNo ratings yet
- Page Et Al-2014-The Cochrane LibraryDocument120 pagesPage Et Al-2014-The Cochrane LibraryLuis UretaNo ratings yet
- Dual Chamber Versus Single Chamber Ventricular Pacemakers For Sick Sinus Syndrome and Atrioventricular Block.Document89 pagesDual Chamber Versus Single Chamber Ventricular Pacemakers For Sick Sinus Syndrome and Atrioventricular Block.Raul OrtegaNo ratings yet
- Interdental Brushing For The Prevention and Control of Periodontal Diseases and Dental Caries in Adults (Review)Document62 pagesInterdental Brushing For The Prevention and Control of Periodontal Diseases and Dental Caries in Adults (Review)Roxana IoneteNo ratings yet
- Jurnal 1Document104 pagesJurnal 1Zayed NorwantoNo ratings yet
- Leyden Et Al-2014-The Cochrane LibraryDocument30 pagesLeyden Et Al-2014-The Cochrane LibraryMartin MontesNo ratings yet
- Edwards 2010Document46 pagesEdwards 2010I Made DuniaNo ratings yet
- Surgical CricothyroidotomyDocument1 pageSurgical Cricothyroidotomyintan rosliNo ratings yet
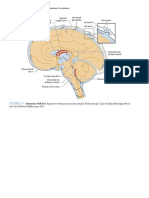
- Figure 3-7: PART I Neuroanatomy and Neuroanatomic LocalizationDocument1 pageFigure 3-7: PART I Neuroanatomy and Neuroanatomic Localizationintan rosliNo ratings yet
- Orthopaedic AnatomyDocument1 pageOrthopaedic Anatomyintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- 7.2 Non-Absorbable Suture MaterialsDocument1 page7.2 Non-Absorbable Suture Materialsintan rosliNo ratings yet
- Antimicrobial Resistance in LeprosyDocument6 pagesAntimicrobial Resistance in Leprosyintan rosliNo ratings yet
- Adolescent Trends and IssuesDocument32 pagesAdolescent Trends and IssuesArleneNo ratings yet
- Status Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPDocument20 pagesStatus Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPpuaanNo ratings yet
- Biosafety and BiosecurityDocument23 pagesBiosafety and BiosecurityMicah LeilaNo ratings yet
- Examination of The AbdomenDocument2 pagesExamination of The AbdomenSetlhare MotsamaiNo ratings yet
- Research SummariesDocument17 pagesResearch Summariesapi-483052208No ratings yet
- Sedation in Pediatric Dentistry: January 2019Document8 pagesSedation in Pediatric Dentistry: January 2019Ina Vetrila100% (1)
- Anemia of Maturation DisordersDocument6 pagesAnemia of Maturation DisordersKim Alyssa GoNo ratings yet
- Cognitive DisorderDocument72 pagesCognitive DisorderJamal P. AlawiyaNo ratings yet
- Tennis ElbowDocument6 pagesTennis ElbowAkshay BangadNo ratings yet
- Result Entry ReportDocument1 pageResult Entry Reportpoojagasti39No ratings yet
- Module 5 Star 2016 - CemerlangDocument59 pagesModule 5 Star 2016 - CemerlangAnna Michael Abdullah75% (8)
- MsdsDocument4 pagesMsdsAdrian MerinoNo ratings yet
- Indian Institute of Technology Delhi Board For Sports ActivitiesDocument4 pagesIndian Institute of Technology Delhi Board For Sports ActivitiessalehknNo ratings yet
- jn.1 Ire CleanDocument6 pagesjn.1 Ire CleanKabakçı HüsnüNo ratings yet
- Low Haemoglobin Density As An Anaemic Indicator in Canine BabesiosisDocument9 pagesLow Haemoglobin Density As An Anaemic Indicator in Canine BabesiosisIndian Journal of Veterinary and Animal Sciences RNo ratings yet
- Post-Operative Complications: Hadi Munib Oral and Maxillofacial SurgeryDocument61 pagesPost-Operative Complications: Hadi Munib Oral and Maxillofacial SurgeryAli ahmedNo ratings yet
- Laboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottDocument29 pagesLaboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottFatah Jati PNo ratings yet
- Swallowing Disorders 2022Document29 pagesSwallowing Disorders 2022Mohammed AhmedNo ratings yet
- 25 Nursing Care of A Family Experiencing A Postpartum ComplicationDocument14 pages25 Nursing Care of A Family Experiencing A Postpartum Complicationmarieekariee777No ratings yet
- "THE LINK" July 2021Document36 pages"THE LINK" July 2021Anonymous SKP0jiK9No ratings yet
- D Aso 81-86Document7 pagesD Aso 81-86Academecian groupNo ratings yet
- Mendel Biology Mock ExamDocument3 pagesMendel Biology Mock Examopeyemi ajayiNo ratings yet
- DHJ 26.04.23 Lengkap ADocument23 pagesDHJ 26.04.23 Lengkap AMalik TeamNo ratings yet
- Chronic Kidney Disease Malaysian CPG 2011Document22 pagesChronic Kidney Disease Malaysian CPG 2011aideeh31100% (1)
- COVIEDDocument11 pagesCOVIEDtahani tttNo ratings yet
- Module 11. Respiratory System17-18Document12 pagesModule 11. Respiratory System17-18Kim RamosNo ratings yet
- Health Unit PlanDocument77 pagesHealth Unit Planapi-658575880No ratings yet