You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dermatological AgentsDocument14 pagesDermatological AgentsHans TrishaNo ratings yet
- FNP Lec Lecture Dec 11Document4 pagesFNP Lec Lecture Dec 11Hans TrishaNo ratings yet
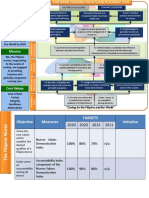
- Vision 2030: "Caring For The Filipino and The World"Document7 pagesVision 2030: "Caring For The Filipino and The World"Hans TrishaNo ratings yet
- Nursing Science and Profession: As An ArtDocument45 pagesNursing Science and Profession: As An ArtHans TrishaNo ratings yet
- Philippine Nursing Act of 2002Document22 pagesPhilippine Nursing Act of 2002Hans TrishaNo ratings yet
- Nursing Code of EthicsDocument28 pagesNursing Code of EthicsHans TrishaNo ratings yet
- Complete Bed Bath RationalesDocument7 pagesComplete Bed Bath RationalesHans TrishaNo ratings yet
- Omplementary AND Lternative HerapiesDocument24 pagesOmplementary AND Lternative HerapiesHans TrishaNo ratings yet
- Client Teaching Infection PreventionDocument2 pagesClient Teaching Infection PreventionHans TrishaNo ratings yet
- CBB ProcedureDocument10 pagesCBB ProcedureHans TrishaNo ratings yet
- Asepsis and Infection ControlDocument139 pagesAsepsis and Infection ControlHans TrishaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 8.V2 (4) 310 319Document10 pages8.V2 (4) 310 319台灣中風醫誌No ratings yet
- Modul 1. Patofisiologi ACSDocument24 pagesModul 1. Patofisiologi ACSFadhilAfifNo ratings yet
- Chapter 24: Alterations of Cardiovascular Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionDocument20 pagesChapter 24: Alterations of Cardiovascular Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionmonicaNo ratings yet
- Spinal Cord Disease by GadisaDocument95 pagesSpinal Cord Disease by GadisaGadisa DejeneNo ratings yet
- Capture The Fracture - Use of Bone Turnover MarkerDocument7 pagesCapture The Fracture - Use of Bone Turnover MarkergusdeNo ratings yet
- Antialergi Dan AnafilaksisDocument14 pagesAntialergi Dan Anafilaksisshofa nur rahmannisaNo ratings yet
- SPICTDocument1 pageSPICTDiklatpimempat Angkatanlimabelas100% (1)
- Melagyn: Effective Intimate HygieneDocument4 pagesMelagyn: Effective Intimate HygieneMohamed AfifyNo ratings yet
- Kode Pintar Icd 10Document60 pagesKode Pintar Icd 10Nur LailaNo ratings yet
- Assessment of LymphadenopathyDocument69 pagesAssessment of LymphadenopathyhiNo ratings yet
- Xyngular Ingredient BenefitsDocument18 pagesXyngular Ingredient BenefitsAnthony RodriguezNo ratings yet
- 17 Ways To Protect Body Mind From Deadly Chronic InflammationDocument36 pages17 Ways To Protect Body Mind From Deadly Chronic Inflammationjazzyz100% (1)
- Certificate of Disability Form-VI PDFDocument3 pagesCertificate of Disability Form-VI PDFpyro_pradeepNo ratings yet
- Lung Cancer: By: Ivan Emmanuel BokingkitoDocument51 pagesLung Cancer: By: Ivan Emmanuel BokingkitoIvanNo ratings yet
- Cholelithiasis SampleDocument77 pagesCholelithiasis Samplekrischamcute67% (3)
- Cellular Aberration Reviewer 5-6Document9 pagesCellular Aberration Reviewer 5-6Jessica A. BurgosNo ratings yet
- Day 9 ASSIGNMENT SDDocument3 pagesDay 9 ASSIGNMENT SDashwinNo ratings yet
- Drugs Used in AneasthesiaDocument73 pagesDrugs Used in AneasthesiaCabdiladif Ahmed McrfNo ratings yet
- Deficient, and 30% of This Group Progresses To Iron-Deficiency AnemiaDocument5 pagesDeficient, and 30% of This Group Progresses To Iron-Deficiency AnemiaTaeyomiNo ratings yet
- MJDF John NabilDocument50 pagesMJDF John NabilAyesha Awan67% (3)
- Inclusiveness - Chapter OneDocument22 pagesInclusiveness - Chapter OneFena Ad100% (1)
- AnthraxDocument27 pagesAnthraxSantosh BhandariNo ratings yet
- Clinical Review: Brash Syndrome: Bradycardia, Renal Failure, Av Blockade, Shock, and HyperkalemiaDocument8 pagesClinical Review: Brash Syndrome: Bradycardia, Renal Failure, Av Blockade, Shock, and HyperkalemiaSyed Shahrul Naz SyedNo ratings yet
- DSM 5 ChartDocument7 pagesDSM 5 ChartJose Luis Gonzalez Celis100% (1)
- Homeopathic Repertory of Modern Drugs Volume III Completo 2 Ed 2021Document808 pagesHomeopathic Repertory of Modern Drugs Volume III Completo 2 Ed 2021Mohit KanjwaniNo ratings yet
- CASE Report Basal Cell Carsinoma of NoseDocument22 pagesCASE Report Basal Cell Carsinoma of NoseDestar Aditya SadegaNo ratings yet
- Clinical Approach To Optic Neuropathies: DiagnosisDocument14 pagesClinical Approach To Optic Neuropathies: Diagnosiskmathewjames100% (1)
- Arte y ReumatologíaDocument7 pagesArte y ReumatologíaMiguel Ángel AlfaroNo ratings yet
- CardiologyDocument88 pagesCardiologyAlshare NisreenNo ratings yet
- Sample Questions 2019Document21 pagesSample Questions 2019kimwell samson100% (1)