You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Robert Kraft - Sample Allegation StoryDocument3 pagesRobert Kraft - Sample Allegation Storyapi-457917734No ratings yet
- Measuring Performance: Guia Mae B. LopezDocument19 pagesMeasuring Performance: Guia Mae B. Lopezgoweb developerNo ratings yet
- 6 Dimensions Procurement ModelDocument9 pages6 Dimensions Procurement ModelMahdi DabarNo ratings yet
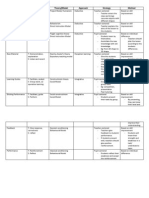
- Steps P&P Theory/Model Approach Strategy MethodDocument2 pagesSteps P&P Theory/Model Approach Strategy Methodlittle large2No ratings yet
- Demo Lesson Plan in Oral Comm.Document3 pagesDemo Lesson Plan in Oral Comm.Kathleen WendeeNo ratings yet
- Organizational Culture Views of ExcellenceDocument25 pagesOrganizational Culture Views of ExcellenceElia Kim FababeirNo ratings yet
- Alumni Form (Responses)Document6 pagesAlumni Form (Responses)Dinda KiranaNo ratings yet
- RSA ANIMATE: Changing Education ParadigmsDocument9 pagesRSA ANIMATE: Changing Education ParadigmsJung Rae SunNo ratings yet
- Santiago v. COMELEC Case DigestDocument5 pagesSantiago v. COMELEC Case Digestrachel cayangaoNo ratings yet
- Depreciation Chart 11-12 (FY)Document4 pagesDepreciation Chart 11-12 (FY)specky123100% (1)
- College of Education Preliminary ExaminationDocument5 pagesCollege of Education Preliminary ExaminationalexNo ratings yet
- EPM v. RolfeDocument30 pagesEPM v. RolfeJudd LegumNo ratings yet
- 6 CA 1 My HUMSS PORTFOLIODocument28 pages6 CA 1 My HUMSS PORTFOLIOCarlitos Malabonga81% (21)
- Mariana Napolitan I: Work Experience Personal BackgroundDocument8 pagesMariana Napolitan I: Work Experience Personal BackgroundArnas Satria HaripanNo ratings yet
- Arsenio Santos Memorial Elementary SchoolDocument5 pagesArsenio Santos Memorial Elementary SchoolCel Rellores SalazarNo ratings yet
- Mobile Services: Your Account Summary This Month'S ChargesDocument7 pagesMobile Services: Your Account Summary This Month'S Chargeslingesh MukilanNo ratings yet
- Cristina Ramirez ResumeDocument1 pageCristina Ramirez Resumeapi-530840537No ratings yet
- A The Preliminary Research and Proposal PhaseDocument39 pagesA The Preliminary Research and Proposal Phaseliam mcphearsonNo ratings yet
- Introduction to History: Defining the PastDocument26 pagesIntroduction to History: Defining the PastYael EzraNo ratings yet
- People v. TulinDocument1 pagePeople v. TulinAnonymous 5MiN6I78I0100% (1)
- SLIDES 3 MarketingDocument18 pagesSLIDES 3 MarketingBibi Shafiqah Akbar ShahNo ratings yet
- Dear Stund I Found An InformationDocument9 pagesDear Stund I Found An InformationAbelito NahasonNo ratings yet
- My Quizzer in Criminology A Reviewer Series IIIDocument260 pagesMy Quizzer in Criminology A Reviewer Series IIIKhael BurerosNo ratings yet
- Aro Barrackpore Rally Notfn 2021Document15 pagesAro Barrackpore Rally Notfn 2021jayanta naskarNo ratings yet
- Principles of Self Management - Strengthening Anticipation, Deliberation, and Stress ToleranceDocument10 pagesPrinciples of Self Management - Strengthening Anticipation, Deliberation, and Stress ToleranceNigel A.L. BrooksNo ratings yet
- Lesson Plan 21Document2 pagesLesson Plan 21Robertson Sondoh JrNo ratings yet
- Critical Analysis of NIA Act AmendmentsDocument8 pagesCritical Analysis of NIA Act AmendmentsAadhitya NarayananNo ratings yet
- Bosch Sistem Digital Traducere Simultana Integrus PDFDocument16 pagesBosch Sistem Digital Traducere Simultana Integrus PDFIoan TrifuNo ratings yet
- B2+ Study Skills Answer KeyDocument1 pageB2+ Study Skills Answer KeyOlgaNo ratings yet
- Prototype ModelDocument17 pagesPrototype ModelKaoboy Nawa LwdeNo ratings yet