You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Module 1 NCM 116 Supplementary ReadingDocument18 pagesModule 1 NCM 116 Supplementary ReadingDjameica Guerrero100% (1)
- Module 3Document6 pagesModule 3Djameica GuerreroNo ratings yet
- NCM 116 Module 2Document17 pagesNCM 116 Module 2Djameica GuerreroNo ratings yet
- Chapter 1Document7 pagesChapter 1Djameica GuerreroNo ratings yet
- Module 2Document6 pagesModule 2Djameica GuerreroNo ratings yet
- Presentation, Analysis and Interpretation of DataDocument11 pagesPresentation, Analysis and Interpretation of DataDjameica GuerreroNo ratings yet
- Summary, Conclusions and RecommendationsDocument5 pagesSummary, Conclusions and RecommendationsDjameica GuerreroNo ratings yet
- Review of Literature and StudiesDocument5 pagesReview of Literature and StudiesDjameica GuerreroNo ratings yet
- Tetanus: Guerrero, Djameica Danielle RDocument16 pagesTetanus: Guerrero, Djameica Danielle RDjameica GuerreroNo ratings yet
- Health History and Physical Assessment On Patient With COPDDocument4 pagesHealth History and Physical Assessment On Patient With COPDDjameica GuerreroNo ratings yet
- Blood Tests: Electrolytes (Sodium, Potassium and Chloride), Urea, Creatinine (Euc)Document5 pagesBlood Tests: Electrolytes (Sodium, Potassium and Chloride), Urea, Creatinine (Euc)Djameica GuerreroNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Comparison Studies of Moringa Oleifera's Seed Powder and Leaf PowderDocument271 pagesComparison Studies of Moringa Oleifera's Seed Powder and Leaf PowderFahad SiddiquiNo ratings yet
- Type 2 DiabetesDocument9 pagesType 2 DiabetesLevi MwendaNo ratings yet
- Manuscript Chapter 1 3Document24 pagesManuscript Chapter 1 3Kira FumiyoshiNo ratings yet
- Health Management of Ewes During Pregnancy: Animal Reproduction ScienceDocument15 pagesHealth Management of Ewes During Pregnancy: Animal Reproduction ScienceAlexander Cañar RomeroNo ratings yet
- 01 EnergeticsDocument10 pages01 EnergeticsUmar Ilyasu JibrilNo ratings yet
- Preventing CancerDocument7 pagesPreventing CancerjelissaNo ratings yet
- ARTISTRY SKNNTN RenewingFirming enDocument55 pagesARTISTRY SKNNTN RenewingFirming enNutellaNo ratings yet
- Bahasa Inggris IlyasDocument4 pagesBahasa Inggris IlyasPuti Citra CantikaNo ratings yet
- Exercise-I: Only One Correct TypeDocument4 pagesExercise-I: Only One Correct TypeMohini DeviNo ratings yet
- Report of Field Attchment at Agriculture Training Centre Machakos From 15 January To 6 APRIL 2018Document17 pagesReport of Field Attchment at Agriculture Training Centre Machakos From 15 January To 6 APRIL 2018Sagini KevinNo ratings yet
- BOYD - TB - 04 FINAL RevDocument29 pagesBOYD - TB - 04 FINAL RevAlyssaNo ratings yet
- Label The Parts of The Plant Cell BelowDocument1 pageLabel The Parts of The Plant Cell BelowEllah MaeNo ratings yet
- A Comprehensive Review of Beetroot Beta Vulgaris L. Bioactive Components in The Food and Pharmaceutical IndustriesDocument33 pagesA Comprehensive Review of Beetroot Beta Vulgaris L. Bioactive Components in The Food and Pharmaceutical IndustriesomaragronomieNo ratings yet
- Test Bank For Textbook of Biochemistry With Clinical Correlations 7th Edition Thomas M DevlinDocument3 pagesTest Bank For Textbook of Biochemistry With Clinical Correlations 7th Edition Thomas M DevlinJames Carson100% (28)
- The Ultimate Anabolic Shake 2Document34 pagesThe Ultimate Anabolic Shake 2Алексей СеменовNo ratings yet
- Mixing Blanding. Straining and RollingDocument5 pagesMixing Blanding. Straining and RollingK cNo ratings yet
- HTP Module 20 Technical NotesDocument91 pagesHTP Module 20 Technical NotesGoytom NeayeNo ratings yet
- The 7 Step Process of Nutrition CoachingDocument25 pagesThe 7 Step Process of Nutrition CoachingMargarida MachadoNo ratings yet
- Biodiversidade de Plantas Alimentícias Não Convencionais em Uma Horta Comunitária Com Fins EducativosDocument17 pagesBiodiversidade de Plantas Alimentícias Não Convencionais em Uma Horta Comunitária Com Fins EducativosMaria ClaraNo ratings yet
- ThesisDocument46 pagesThesisNasser NarcisoNo ratings yet
- Ben - Morgan A Case of Diabetes 2Document2 pagesBen - Morgan A Case of Diabetes 2api-463462603No ratings yet
- Tristin Geschwender - ResumeDocument2 pagesTristin Geschwender - Resumeapi-534459504No ratings yet
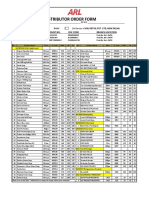
- Order Form December 2021Document1 pageOrder Form December 2021Ravi JoshiNo ratings yet
- Bài Tập Bổ Trợ Family and FriendsDocument8 pagesBài Tập Bổ Trợ Family and FriendsChâu KýNo ratings yet
- The Top Fiber-Rich Foods ListDocument8 pagesThe Top Fiber-Rich Foods ListSabina Alic100% (1)
- Zotrim Brand Promotional GuideDocument11 pagesZotrim Brand Promotional GuideCelas ChilliesNo ratings yet
- 1653 3071 1 SMDocument21 pages1653 3071 1 SMTau GakNo ratings yet
- National Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024Document78 pagesNational Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024rukwavuNo ratings yet
- Grains: Whole-Wheat Bread (Roti) Whole-Wheat Bread T (Aata Bread)Document23 pagesGrains: Whole-Wheat Bread (Roti) Whole-Wheat Bread T (Aata Bread)Ashish GoelNo ratings yet
- CARBOHYDRATESDocument31 pagesCARBOHYDRATESCheelsy P. ButronNo ratings yet