Professional Documents
Culture Documents
Management of Gastric Polyps: A Pathology-Based Guide For Gastroenterologists
Uploaded by
cc vereOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Management of Gastric Polyps: A Pathology-Based Guide For Gastroenterologists
Uploaded by
cc vereCopyright:
Available Formats
reviews
Management of gastric polyps: a pathology-
based guide for gastroenterologists
Susanne W. Carmack, Robert M. Genta, David Y. Graham and Gregory Y. Lauwers
abstract | 1–4% of patients who undergo gastric biopsy have gastric polyps. These lesions may be true
epithelial polyps, heterotopias, lymphoid tissue, or stromal lesions. Hyperplastic polyps, which arise in
patients with underlying gastritis, and fundic-gland polyps, which are associated with PPi therapy, are the most
common gastric polyps; however, prevalence varies widely relative to the local prevalence of Helicobacter
pylori infection and use of PPi therapy. some polyps have characteristic topography, size, and endoscopic
appearance. Approximately 20% of biopsy specimens identified endoscopically as polyps have no definite
pathological diagnosis. evaluation of the phenotype of the gastric mucosa that surrounds a lesion will provide
significant information crucial to the evaluation, diagnosis and management of a patient. The presence of
a gastric adenoma should prompt the search for a coexistent carcinoma. The endoscopic characteristics,
histopathology, pathogenesis, and management recommendations of polyps and common polypoid lesions in
the stomach are discussed in this review.
Carmack, s. w. et al. Nat. Rev. Gastroenterol. Hepatol. 6, 331–341 (2009); published online 5 May 2009; doi:10.1038/nrgastro.2009.70
Classic studies and the majority of textbooks on gastro
Continuing Medical Education online
intestinal pathology indicate that although adenoma
This activity has been planned and implemented in accordance tous polyps1 have a high malignant potential and are
with the essential Areas and policies of the Accreditation frequently associated with synchronous gastric adeno
Council for Continuing Medical education (CMe) through the joint
carcinomas, risk of malignant transformation is very low
sponsorship of Medscape, LLC and Nature Publishing Group.
for hyperplastic gastric polyps and is virtually absent
Medscape, LLC is accredited by the Accreditation Council for
Continuing Medical education (ACCMe) to provide continuing in sporadic fundicgland polyps (FGPs).2 as a conse
medical education for physicians. quence, the diagnosis of an adenomatous gastric polyp
Medscape, LLC designates this educational activity for a maximum may trigger inclusion of the patient into an endoscopic
of 1.0 aMa pra Category 1 CreditstM. Physicians should only claim surveillance program, whereas only limited followup is
credit commensurate with the extent of their participation in the generally proposed for patients with diagnoses of hyper
activity. All other clinicians completing this activity will be issued
a certificate of participation. To participate in this journal CMe plastic polyps, inflammatory polyps, or FGPs.3 However,
activity: (1) review the learning objectives and author disclosures; molecular studies contest this longheld management
(2) study the education content; (3) take the post-test and/or approach. Gastric polyps other than adenomatous
complete the evaluation at http://cme.medscape.com/public/
polyps display molecular alterations that may lead to
naturereviews; and (4) view/print certificate.
neoplastic progression, and might carry unknown risks veterans Affairs North
learning objectives of malignant transformation. Texas Health Care
Upon completion of this activity, participants should be able to: system, University of
1 List the variables associated with a higher rate of gastric southwestern Medical
adenoma.
Clinical and pathological correlations Center, Dallas, TX, UsA
2 identify the endoscopic features of different gastric polyps. substantial information on the etiology of a gastric (s. W. Carmack,
r. M. genta).
3 identify the histologic features of different gastric polyps. polyp or lesion and correlations between clinical and Michael e. DeBakey
4 Describe the appropriate management of different gastric pathological findings can be gathered by histological veterans Affairs
polyps. Medical Center, Baylor
and pathological evaluation of an appropriately College of Medicine,
representative range of biopsy samples taken from the Houston, TX, UsA
unaffected gastric mucosa. (D. y. graham).
Massachusetts
Introduction although most gastroenterologists are aware of the General Hospital,
most biopsy specimens of presumed gastric polyps value of examining the mucosa that surrounds a gastric Harvard Medical
school, Boston, MA,
have distinctive clinical characteristics that enable their polyp or lesion, in our experience a thorough examina UsA (g. y. lauwers).
easy categorization into one of the major established tion of the affected gastric mucosa is not commonly
classes of epithelial or stromal gastric lesions (table 1). performed at the time a polyp is discovered. the clini Correspondence:
r. M. Genta, Caris
cal characteristics of gastric polyps or lesions, and the Diagnostics, 8400
possible pathological findings of the gastric mucosa esters Blvd, irving,
Competing interests TX 75063, UsA
The authors, the Locum Journal editor r. Jones and the CMe adjacent to these entities, are highlighted in tables 2 robert.genta@
questions author C. P. vega declare no competing interests. and 3. utsouthwestern.edu
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 331
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
Key points polyps, because not all polyps may have been described
and excised.5,6
■ Multiple entities may present as a gastric polypoid lesion, and many have
subtle yet characteristic endoscopic features similarly to other gastric diseases, important geo
graphical differences in the prevalence of gastric polyps
■ in western countries, fundic-gland polyps are now more common than
hyperplastic polyps, resulting from the increase in PPi therapy and decrease in exist. rates of gastric adenomas and adenocarcinomas
gastritis associated with Helicobacter pylori infection are much higher in eastern europe and asia than in
■ Biopsy specimens of the gastric mucosa adjacent to a lesion are extremely western populations, with figures approaching 27%
important in establishing an etiology when hyperplastic polyps, adenomas, and compared with 0.5–3.75%, respectively.7–9 a retrospec
carcinoids are present tive review of 13,000 endoscopies performed on Greek
■ surveillance is indicated in patients with polyposis syndromes and adenomas; adults yielded 258 gastric polyps (1.2%).5 up to 27% of
patients with gastrointestinal stromal tumors and carcinoids may be followed patients had more than one polyp, and 75.6% had hyper
up endoscopically, but management approach should be tailored to each plastic polyps. adenomas (6.6% of all polyps) were pre
individual dominantly found in males (2:1 male to female ratio),
and were found only in patients over 50 years of age.
stromal polyps were present in 5.2% of patients who
Table 1 | Classification of gastric polyps and polypoid lesions had previously undergone gastrectomy or gastrojejuno
Classification polyp or lesion stomy. a large, pathologybased, German study ana
Neoplastic Adenomatous carcinoma (primary or metastatic)
lyzed 5,515 gastric polyps collected between 1969 and
Carcinoid 1989 and found 47% to be FGPs and 28.3% to be hyper
Hyperplastic or Usual (gastritis-related)
plastic polyps; high representations of gastric adenomas
inflammatory Polypoid hyperplasia near sites of repair (i.e. stomas, ulcers) (9.0%) and adenocarcinomas (7.2%) were found.4 a
Cardiac (reflux) 2007 Brazilian study of the findings of 26,000 endo
inflammatory fibroid polypa scopies identified a mere 153 patients with gastric polyps
Hamartomatous or Fundic-gland polypa (0.58%). the relative frequency of polyps in this popula
developmental Peutz–Jeghers tion reflected the high rate of H. pylori infection: 71.3%
Juvenile
Cowden disease
of polyps were hyperplastic polyps, 16.3% were FGPs,
Pancreatic heterotopia and 12.4% were gastric adenomas.6 recently, we exam
Mesenchymal Gastrointestinal stromal tumor ined data on gastric polyps obtained over a 12month
smooth-muscle tumors period in a nationwide pathology laboratory in the
Glomus tumor us.10 in approximately 200,000 patients who underwent
Neural tumors (schwannoma/neuroma, ganglioneuroma, esophago gastroduodenoscopy (eGD), 8,000 gastric
granular-cell tumor)
polyps were excised or biopsied from 7,500 patients, with
Miscellaneous Xanthoma an overall gastricpolyp prevalence of 3.75%—somewhat
Lymphoid hyperplasia or lymphoma
Hemangioma or lymphangioma higher than the amount previously reported for western
a
Considered benign, but genetic mutations are common.
populations. in this population with a low prevalence
of H. pylori infection (12.3% among the 78,909 patients
who had gastric biopsies), the overwhelming major
Epidemiology ity of gastric polyps (77.2%) were FGPs, 14.4% were
Published data on the epidemiology of gastric polyps inflammatory or hyperplastic polyps, and only 0.7%
diverge substantially with regard to both absolute and were gastric adenomas.
relative prevalence. among the variables that influence
epidemiological data, we must consider the populations Classification and key features
studied, which will have wide variations in age and sex, a diverse array of polyps and polypoid lesions may be
and the prevalence of underlying gastric conditions, such found in the stomach. table 1 illustrates the various
as Helicobacter pylori infection. the methodology of entities that may appear endoscopically as a polyp or
studies and the accuracy of pathological diagnoses should nodule. epithelial polyps (hyperplastic, fundic gland, and
also be considered. thus, we must be aware that we are adenomatous) are the classic gastric polyps, but clusters
comparing unevenly obtained data. a detailed discus of endocrine cells (carcinoids), infiltrates (xanthomas,
sion on the effects of these variables is beyond the scope lymphoid proliferations) or mesenchymal prolifera
of this review, but it should be noted that problems exist tions (gastrointestinal stromal tumors [Gists], leio
with the two most common types of studies: pathology myoma and inflammatory fibroid polyps) may produce a
based series and retrospective studies. Pathologybased mucosal protrusion. this review excludes discussion of
series, in which the denominator is the total of gastric carcinomas, lymphomas, and other malignancies.
biopsy samples available, cannot be used to establish the
absolute prevalence of gastric polyps, but are adequate Fundic-gland polyps
to determine the relative frequency of the various types Clinical characteristics
of polyps.4 retrospective reviews of endoscopic reports FGPs are the most common type of polyp detected
are likely to underestimate the true prevalence of gastric by eGD in western countries. 10 endoscopically they
332 | JUNE 2009 | volUmE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
Table 2 | Clinical characteristics of gastric polyps
polyp type prevalence gastric location size endoscopic appearance pathological Comments
(frequency features of
relative to background
other polyps) gastric mucosa
Fundic gland 13–77% Fundus and upper <1 cm smooth, glassy, transparent; Helicobacter Associated with PPi
body usually multiple polyps are pylori-associated use; may regress;
found gastritis is rare dysplasia found in
patients with FAP
Hyperplastic 18–70% random, adjacent Generally small polyps have a smooth Atrophic gastritis with Found in patients with
to ulcers or stoma <1 cm dome; large polyps are intestinal metaplasia; gastritis; dysplasia is
sites, or in the lobulated, and erosions Helicobacter rare (<3%) and found in
cardia if related are common pylori-associated polyps <2 cm
to acid reflux gastritis (25%)
Adenoma 0.50–3.75% Incisura angularis, <2 cm velvety, lobular surface; Atrophic gastritis with May be accompanied by
(in western found more in the exophytic, sessile or intestinal metaplasia coexistent carcinoma
hemisphere) antrum than pedunculated; usually
fundus solitary (82%)
inflammatory 0.1–3.0% submucosal, Median 1.5 cm; single, firm, sessile, Pernicious anemia etiology is believed
fibroid found near the generally <3 cm well-circumscribed, commonly found; to be reactive, but
pyloric sphincter ulceration is common atrophic gastritis genetic mutations
are common
Peutz–Jeghers rare random <1 cm Pedunculated with a velvety Normal risk of
or papillary surface adenocarcinoma, but
rare in gastric polyps
Juvenile rare Found more in variable More rounded than Normal Polyps may exclusively
the body than hyperplastic polyps; involve stomach; risk of
in the antrum superficial erosions; multiple adenocarcinoma but
polyps are usually found rare in gastric polyps
Abbreviations: FAP, familial adenomatous polyposis; MeN, multiple endocrine neoplasia; Zes, Zollinger–ellison syndrome.
Table 3 | Clinical characteristics of gastric polypoid lesions
polypoid lesion prevalence gastric location size endoscopic appearance pathological Comments
(frequency features of
relative to background
other polyps) gastric mucosa
Xanthoma 0.3–3.9% Antrum, lesser <3 mm Can be multiple in groups; Chronic gastritis No association with
curvature, sessile, pale-yellow nodule hyperlipidemia. Lesions
prepyloric or plaque represent a reparative
response
Pancreatic 0.80% Antrum, prepyloric 0.2–4.0 cm solitary; dome-shaped Normal very rare instances of
heterotopia with central dimple; associated pancreatitis,
smooth surface islet-cell tumors,
adenocarcinoma
Gastrointestinal 1% of all random, variable well-circumscribed; Normal 25% are malignant:
stromal tumor gastrointestinal submucosal (median 6 cm) overlying mucosa may risk of aggressive
malignancies be ulcerated behavior depends on
size and mitotic count
Carcinoid <0.5% Body and fundus <2 cm, larger if Hypergastrinemic lesions: Autoimmune atrophic Associated with
sporadic firm, yellow, broad-based gastritis with intestinal hypergastrinemia,
and multiple metaplasia; parietal autoimmune atrophic
sporadic lesions: cell hyperplasia in gastritis, Zes or MeN
large and single Zes; normal mucosa
if lesion is sporadic
Abbreviations: MeN, multiple endocrine neoplasia; Zes, Zollinger–ellison syndrome.
appear as smooth, glassy, sessile, circumscribed eleva recognize when markedly dilated (Figure 1b,c). FGPs
tions (usually measuring <0.5 cm) in the oxyntic mucosa may occur sporadically, in association with PPi use, and
(Figure 1a). Histologically, the basic lesion consists of in patients with familial adenomatous polyposis (FaP)
one or more cystically dilated oxyntic glands, with syndrome.11–13 sporadic polyps are either single or few
the lining cells appearing flattened and difficult to in number, and are found almost exclusively in patients
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 333
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
a b c
p
p
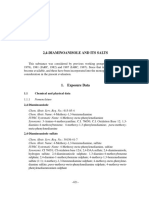
Figure 1 | A fundic-gland polyp. a | endoscopically, they appear as glassy, smooth, round polyps (often multiple) in the
gastric body and fundus. b | A low-power histological view displaying dilated glands that may be lined by parietal cells (p) or
mucous cells (m). c | A high-power histological view showing both flattened parietal cells (thin black arrows) and mucous
cells (thick black arrow).
without H. pylori infection.14 in PPi users, large numbers and surveillance endoscopy from the time of initial
of polyps might exist, but these may regress with cessa colonoscopy, irrespective of referable symptoms.13
tion of therapy.15 little is known about the etiology of when multiple FGPs are diagnosed in a young patient,
FGPs. in the past, these polyps were considered to be FaP should be considered. the responsibility of alerting
hamartomatous; however, the recognized association the clinician to this possibility and performing a careful
of FGPs with longterm PPi use suggests that mech search for dysplasia is incumbent upon a conscientious
anisms related to the suppression of acid secretion may pathologist. no immunohistochemical or molecular
be involved in their pathogenesis.16,17 However, this view studies are warranted outside a research setting.
is not shared by all researchers.18,19 our understanding
of the pathogenesis of these polyps has been further hyperplastic polyps
complicated by the finding that sporadic FGPs with dys Clinical characteristics
plasia exhibit germline mutations in the APC tumor Hyperplastic polyps arise most frequently in patients
suppressor gene (a finding also observed in patients with with an inflamed and often atrophic gastric mucosa.24
FaP),20 rather than somatic mutations in the βcatenin in the industrialized world, both their absolute and rela
gene, which had previously been described in association tive prevalence has decreased along with the declining
with these polyps.21,22 prevalence of H. pylori infection.25
Hyperplastic polyps are more frequently observed in
Management the antrum than in other parts of the stomach and are
although dissenting opinions have been expressed, spor often multiple; these polyps are usually smooth, dome
adic and PPiassociated FGPs are traditionally believed shaped and small in diameter (measuring 0.5–1.5 cm),
to have low malignant potential and no ominous associ but they may reach much larger dimensions, wherein
ations.23 in patients on PPi therapy with typical, small they become lobulated and pedunculated (Figure 2a).26 in
(<0.5 cm) FGPs, diagnosis is confirmed by taking a larger hyperplastic polyps, the surface epithelium is often
biopsy specimen from one polyp. Biopsy specimens are eroded. this erosion may result in chronic blood loss
taken from all polyps 0.5–1.0 cm in size. PPi therapy is and irondeficiency anemia, one of the most common
not discontinued in patients with smaller polyps. larger clinical manifestations of hyperplastic polyps. rarely,
polyps (>1 cm) are removed and, if clinically appropriate, patients with large hyperplastic polyps may present with
PPi therapy is discontinued in these patients. By contrast, gastric obstruction.27,28
a definite risk of dysplasia (between 30% and 50%) is Histologically, hyperplastic polyps consist of elongated,
present in FaPassociated FGPs.11 in a 2008 study of 75 grossly distorted, branching and dilated hyperplastic
patients undergoing surveillance for FaP, 88% had FGPs, foveolae lying in an edematous stroma rich in vascula
38% had lowgrade dysplasia and 3% had highgrade ture, and small, haphazardly distributed smoothmuscle
dysplasia.12 Dysplasia in FGPs was associated with large bundles; they contain varying degrees of chronic and
polyp size (>1 cm), increased severity of duodenal poly active inflammation (Figure 2b,c). owing to this often
posis, and antral gastritis. PPi therapy use seemed to have prominent inflammatory component, some clinicians and
a protective effect against dysplasia in FGPs. although no researchers prefer the term hyperplasticinflammatory
official guidelines have been issued, the general consen polyps to hyperplastic polyps, and a few refer to them
sus is that all pediatric, and perhaps also adult, patients simply as inflammatory polyps. some confusion has
with FaP warrant upper gastrointestinal screening resulted from these loosely interchanged terms.
334 | JUNE 2009 | volUmE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
a b c f
Figure 2 | A hyperplastic polyp. a | An endoscopic view showing lobulations with an irregular surface. b | A low-power
histological view showing irregular, distorted, branching foveolae, which may form mucous-cell-lined cysts (m); the
stroma is vascular and edematous with chronic and active inflammation. c | A high-power histological view showing an
eroded branch of a hyperplastic polyp. The epithelial surface is replaced by a thick deposit of fibrin (f), which overlays
a richly vascular granulation tissue. such erosions, which are universal in larger polyps, often result in blood loss and
iron-deficiency anemia.
a hyperproliferative response to tissue injury (erosions when a hyperplastic polyp of any size, with or without
or ulcers) accompanied by increased cellular exfoliation dysplasia, is diagnosed, a full set of topographically
results in the histopathological appearance of fove defined biopsy specimens (‘gastric mapping’) should be
olar hyperplasia.29 Foveolar hyperplasia has long been obtained. if H. pylori gastritis is present, eradication of
recognized as a prominent feature of chemical gastro H. pylori is warranted with a followup endoscopy after a
pathy (caused by bile reflux or nsaiDs), and to a lesser few months to monitor not only cure of the infection, but
extent in H. pylori gastritis.30 Polypoid foveolar hyper also recurrence or regression of remaining polyps.31,32 if
plasia, gastric foveolar polyps, gastritis cystica polyposa extensive atrophy and metaplasia are found, the patient
(characteristic of postBillroth i and ii gastric stumps), should be considered at risk for gastric cancer, as the
and gastric hyperplastic polyps are considered variants of polyp could be viewed as an alarming lesion, and an
the same basic hyperproliferative disturbance. individualized surveillance plan (for which guidelines
do not yet exist) should be implemented.24 if the polyp
Management is obtained from a gastrectomy site in the absence of
removal of the underlying injury (that is, eradication of dysplasia, optimal management remains uncertain.
H. pylori infection) results in regression of hyperplastic
polyps in a high proportion of patients (up to 70% in adenomatous polyps
one study).31,32 Clinical characteristics
Both isolated hyperplastic polyps and the polypoid adenomatous polyps may occur sporadically and in
lesions found at gastrectomy sites have a low but definite association with FaP. only the former are discussed
potential for development of malignancy. Between 1% in this review. endoscopically, adenomatous polyps
and 20% of hyperplastic polyps have been found to harbor have a velvety, lobulated appearance, are usually solitary
foci of dysplasia; furthermore, mutations of the p53 gene, (82%), located in the antrum, and <2 cm in diameter
chromosomal aberrations, and microsatellite instability (Figure 3a).1 these polyps are circumscribed lesions,
have been detected in these polyps.33–36 molecular studies pedunculated or sessile and histology will reveal dys
examining these polyps were designed to acquire insights plastic epithelium without detectable invasion of the
into possible neoplastic mechanisms, not to develop pre lamina propria (Figure 3b). their prevalence varies
dictive tests: thus, in the clinical setting, the perform widely and is estimated to be 0.5–3.75% in western
ance of immunostaining to detect p53 accumulation, countries and 9–27% in areas with higher rates of gastric
microsatellite instability testing (both easily available and carcinoma, such as China and Japan.4,7,39
accurate) or gene arrays, would yield results whose full sporadic, gastric adenomatous polyps may be viewed
clinical implications could not be interpreted. the overall as one of the possible steps in the development of gastric
prevalence of dysplasia in hyperplastic polyps is believed adenocarcinoma. Both conditions arise most often in
to be <2%, and more frequent in large polyps (>2 cm).37,38 patients with chronic, atrophic, metaplastic gastritis and
large, hyperplastic polyps should be completely excised they share a common epidemiological pattern. the larger
for thorough histological evaluation. if dysplasia, or even an adenomatous polyp, the greater the probability that it
intramucosal carcinoma, was present, it will have been contains foci of adenocarcinoma. a synchronous adeno
removed and most likely will have been cured. carcinoma in another area of the stomach has been found
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 335
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
a b are easily recognized by their characteristic arborizing
pattern of muscle fibers between hyperplastic glands.44
Management
a detailed discussion of the management of different
polyposis syndromes is beyond the scope of this review.
However, we will summarize the recommendations for
screening and surveillance of the upper gastrointestinal
tract for the three moststudied conditions: FaP, Peutz–
Jeghers syndrome, and juvenile polyposis. the presence
of gastroduodenal polyposis is well recognized in patients
with FaP. However, the dearth of published studies pre
Figure 3 | An adenomatous polyp. a | An endoscopic view showing a velvety
surface. b | A low-power histological view. Not unlike their colonic counterparts,
vents an accurate assessment of the potential benefits
gastric adenomatous polyps are usually exophytic lesions composed of interlacing of surveillance, particularly in light of the relatively low
sheets of irregular tubular epithelium that may form complex structures with a risk of gastric cancer found in these patients in western
cribriform architecture (arrows). Cells are crowded in a disorderly arrangement countries. 47,48 a reasonable management approach
(inset high-power histological view), often elongated, with hyperchromatic nuclei involves the performance of an upper gastrointestinal
and occasional mitoses. Paneth cells, and rarely oxyntic cells, may be found in endoscopy at 3year intervals from 30 years of age, with
various proportions. the aim of detecting early curable cancers. Patients
with large numbers of gastric and duodenal polyps and
in up to 30% of patients with an adenomatous polyp, and those with dysplastic polyps (FGPs with epithelial dys
up to 50% of adenomatous polyps >2 cm harbor a focus plasia and adenomas) are recommended to undergo
of adenocarcinoma.40,41 surveillance yearly.43
individuals with Peutz–Jeghers syndrome are at risk of
Management a wide variety of cancers at a young age, including cancer
the management of gastric adenomas has not been of the breast, colon, pancreas, stomach, small intestine,
markedly changed by molecular studies that have con ovaries, uterus, and testes. the lifetime risk for gastric
firmed their neoplastic nature. a 2003 molecular study cancer has been estimated to be ~30% in patients with
reported that distinction of the type of gastrointestinal Peutz–Jeghers syndrome;49 most authorities, therefore,
adenoma (intestinal versus gastric) might further define suggest surveillance of the stomach and small intestine
the risk of cancer (an increased risk of cancer is associ with upper endoscopy and smallbowel series every
ated with intestinal adenomas). 41 Gastric mapping is 2–3 years, starting at 18 years of age. 50 surveillance
useful to determine the phenotype of gastritis on which should continue every 2–3 years if polyps are noted at
an adenoma arises; the finding of metaplastic atrophic baseline evaluation.43, 51
gastritis is an indication for surveillance.42 in addition, a Juvenile polyposis is rare and data regarding gastric
thorough search for synchronous adenocarcinoma should malignancy are limited. as the risk of gastric cancer in
be performed and the endoscopist should confirm com patients with this condition is estimated to be 15–20%,
plete excision of the adenoma with a repeat endoscopy it seems reasonable to offer gastric endoscopic surveil
if necessary. the guidelines of the american society of lance at intervals of 1–2 years, with simultaneous
Gastrointestinal endoscopy (asGe) recommend endo colonoscopy.43,52
scopic surveillance at 1 year followup for patients with recommendations for the management of Cronkite–
gastric adenoma, and that specific biopsy techniques be Canada syndrome have focused on pharmacological
implemented when large or multiple polyps exist.42 therapy and surgical resection. 53 Cowden disease has
no documented association with gastrointestinal malig
polyposis syndromes nancies; screening is, therefore, aimed at detecting breast
Clinical characteristics and thyroid cancers.54
Polyposis syndromes that affect the stomach are rare, and
patients with these syndromes often present with clini Inflammatory fibroid polyps
cal manifestations unrelated to gastric polyps. However, Clinical characteristics
some cases of juvenile polyposis may affect the stomach inflammatory fibroid polyps (also known as vanek
alone.43,44 the hamartomatous polyps found in juvenile tumors) are rare lesions that represent <1% of all gastric
polyposis, Cronkite–Canada syndrome and Cowden polyps. although these polyps can form throughout
disease have subtle histological findings that closely the gastrointestinal tract, 80% arise in the antropyloric
mimic hyperplastic gastric polyps and might easily be region.55 these polyps are firm, solitary, sessile or pedun
overlooked if the diagnosis is not suggested by the clini culated, and are often ulcerated (Figure 4a); they have
cal context.45,46 Patients with FaP can have FGPs with been associated with hypochlorydia or achlorhydria, as
dysplasia as well as adenocarcinoma. Hamartomatous well as with adenomas.55 inflammatory fibroid polyps
polyps in patients with the Peutz–Jeghers syndrome are usually found incidentally, although symptoms
336 | JUNE 2009 | volUmE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
of bleeding and gastricoutlet obstruction have been a b
reported.56 Histologically, these lesions consist of a sub
mucosal proliferation of spindle cells, small vessels, and
a striking inflammatory infiltrate, in which eosinophils
predominate (Figure 4b). owing to the massive eosino
philic infiltrates, these polyps are occasionally referred
to as eosinophilic granulomas; however, this term is
incorrect, as these polyps are not granulomas and confu
sion might occur with langerhan cell histiocytosis (also
known as eosinophilic granuloma).
the etiology of inflammatory fibroid polyps is
unknown. a familial tendency has been suggested by
researchers, owing to the finding of a family in Devon,
uK, whose female members have a high rate of these
polyps.57 the presence of eosinophils in a lesion is sure to
Figure 4 | An inflammatory fibroid polyp. a | endoscopic view showing a firm,
elicit allergyrelated speculations; however, no support
well-circumscribed, vascular, submucosal polyp. b | A low-power histological view
ive evidence is currently available. immunohistochemical showing a compact aggregate of concentrically organized spindle cell (fibroblasts),
staining suggests these polyps originate in dendritic prominent vascularity and abundant inflammatory cells, predominantly eosinophils
cells.58 the mucosa adjacent to these polyps is often (inset high-power histological view). The surface mucosa might be normal,
unremarkable, but associations with chronic atrophic hyperplastic, or eroded.
gastritis have been reported. a recent study found that
70% of inflammatory fibroid polyps contain gainof
function mutations in the gene encoding PDGFα poly a b
peptide, similar to those found in KITnegative Gists,
which suggests the possibility of a neoplastic process.59
Management
as most inflammatory fibroid polyps are found inci
dentally and do not recur after excision, neither further
treatment beyond local excision nor surveillance is
recommended.60
gastrointestinal stromal tumors
Clinical characteristics Figure 5 | A gastrointestinal stromal tumor. a | An endoscopic view showing a
Gists are rare tumors of the gastrointestinal tract and well-circumscribed, hard, submucosal polyp with normal overlying mucosa. These
comprise 1–3% of gastric neoplasms.61,62 these tumors polyps are often large when detected, and their surface may be ulcerated.
are most commonly found in men and in the gastric b | Histological view (low power) of the tumor. A high-power image (inset) shows
fundus, although they can be found in other regions that the lesion is formed by a compact mass of whirling CD117-positive spindle
cells, which usually infiltrate the submucosa. The overlying mucosa is edematous
of the stomach. the gastric mucosa that surrounds
with distorted glands displaced by the infiltrating neoplastic cells.
these lesions is usually normal. microscopic Gists are
common in the upper stomach of Japanese patients who
have undergone gastric resection for gastric cancers, of cases.61 on the basis of size and mitotic activity, Gists
which suggests that only a few lesions enlarge and are categorized for risk of malignancy (very low risk to
develop malignant potential.63 high risk).
endoscopically, Gists are wellcircumscribed sub
mucosal lesions (median diameter 6 cm) that occa Management
sionally show an eroded or ulcerated overlying mucosa all Gists must be considered as having malignant
(Figure 5a). the gastric mucosa tends to slide over potential, with up to 50% of patients having metastatic
benign, submucosal tumors, which might be missed disease at presentation, usually of the liver.64 in practice,
by the biopsy forceps. thus, representative tissue is a strong correlation exists between the mitotic activity,
best obtained by endosonographic fineneedle aspira size, and clinical behavior of Gists. surgical resection is
tion. Histologically, Gists are composed of spindle cells recommended for lesions >2 cm; endoscopic enucleation
(Figure 5b), in some cases with an epithelioid (rounding followed by surveillance is an option for small Gists.
up) morphology.61 these lesions are believed to originate endoscopic removal is controversial, however, because
from the interstitial cells of Cajal, the gut’s pacemaker of reports of positive resection margins and tumor spill
cells. Gists have unique immunostaining character age.65 tyrosine kinase inhibitors are used as targeted
istics that allow a specific diagnosis: the stain for KIT therapy in cases of metastasis and surgically unresect
gene product, CD117, is positive in approximately 95% able Gists.66 neoadjuvant therapy with use of tyrosine
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 337
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
a b and eClcell hyperplasia. Carcinoids associated with
hypergastrinemia are usually multiple, broadbased,
firm, yellowish lesions located in the body and fundus
of the stomach, and rarely measure >2 cm (Figure 6a).
sporadic carcinoid tumors occur in a normal gastric
mucosa with no apparent associations; they are typi
cally single, tend to be prepyloric, and are usually >2 cm
when detected.71,72
Histologically, carcinoids are composed of nests or
ribbons of endocrine cells (small polygonal cells with
round nuclei featuring ‘salt and pepper’ chromatin)
Figure 6 | A carcinoid. a | An endoscopic view showing the broad-based
(Figure 6b). necrosis, anaplasia, increased mitotic activ
appearance of these polyps with a yellowish tinge. b | A low-power histological view ity, and size >2 cm are markers of aggressive behavior,
showing that these polyps are formed by ribbons and clusters (nests) of small and are found exclusively in sporadic carcinoids.71 the
monotonous cells (clearly visible at higher power [inset]) that displace the normal carcinoid syndrome (which is characterized by cutane
mucosal glands. Larger lesions expand into and beyond the muscularis mucosae. ous flushing, diarrhea, bronchospasm and cardiac valvu
lar lesions) is present almost exclusively in patients with
sporadic carcinoids.70
a b
X
Management
Prognosis and therapy depend on the type of carcinoid.73
X
type i carcinoids rarely metastasize, 5year survival rates
of 95% are reported, and patients may be followed up
X
endoscopically after local excision and biopsy specimens
have been obtained from the surrounding mucosa.72–74
surveillance is not recommended in patients with perni
cious anemia, although according to asGe guidelines,
the performance of one endoscopy is appropriate. 42
Figure 7 | A xanthoma. a | endoscopic view. As their name indicates, xanthomas antrectomy might be considered if a patient has multi
are pale-yellow plaques or nodules, and are often multiple (arrows). b | A low-power ple carcinoids. the prognosis of patients with type ii
histological view showing irregular expansions of the lamina propria (X), which is carcinoids is excellent when the underlying gastrinoma
filled by macrophages laden with foamy-appearing lipids (inset high-power view). can be successfully removed; when this is not possible,
The overlying epithelium is usually made of normal mucosa. endoscopic polypectomy followed by surveillance is the
accepted therapy and management. 75 sporadic carci
kinase inhibitors after surgical resection of highrisk noids behave like neuroendocrine carcinomas, with a
Gists deters recurrence, but the optimal duration of propensity for invasion and metastases. the therapy
therapy remains unknown.67 of choice is gastrectomy, but the 5year survival rate
remains below 50%.68
Carcinoids
Clinical characteristics Xanthomas
Carcinoids comprise less than 2% of gastric polypoid Clinical characteristics
lesions.4,68 the term carcinoid is used here in the tradi Xanthomas (also known as xanthelasmas) are small
tional connotation of a type of neuroendocrine tumor (<3 mm), yellowish nodules or plaques that barely
derived from enterochromaffinlike (eCl) cells.69 three protrude from the surrounding pink gastric mucosa
types of carcinoids are recognized: type i are associated (Figure 7a). these sessile lesions, which rarely attain the
with chronic autoimmune atrophic gastritis (65–80% of size and shape of a polyp, are often found near the site
all gastric carcinoid tumors, female predominance, often of mucosal repair, such as gastrectomy stomas, ulcers,
accompanied by pernicious anemia); type ii are associ or, less commonly, the mucosa adjacent to an adeno
ated with Zollinger–ellison syndrome and multiple carcinoma. Xanthomas are also commonly associated
endocrine neoplasia type 1 (3–15% of tumors); type iii with chronic gastritis and may be found in small clusters
are sporadic (~20% of tumors, male predominance).70 along the lesser curvature, antrum, and prepyloric areas
type i carcinoids are associated with hypergastrinemia, of the stomach. Histologically, they consist of aggre
which results from loss of negative feedback to the gates of lipidladen macrophages that contain chole
G cells in the antrum secondary to the destruction of sterol and neutral fat loosely embedded in the lamina
parietal cells and increasing gastric pH. type ii carci propria (Figure 7b). their prevalence is low in the west;
noids are also associated with hypergastrinemia, but as a however, for unknown reasons, possibly related to the
result of a gastrinoma—a gastrinproducing tumor that high prevalence of chronic gastritis, these lesions are
leads to the development of hypertrophic parietal cells common in asia.76
338 | JUNE 2009 | volUmE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
Xanthomas represent a reparative response and are a b
not associated with hypercholesterolemia. in cases of
chronic gastritis, they might be associated with intestinal
metaplasia and hyperplastic polyps.77
Management
Xanthomas are, in themselves, clinically insignificant
lesions. However, because of their possible associ
ation with other potentially serious conditions of the
stomach, the remainder of the gastric mucosa should be
examined carefully.77
pancreatic heterotopia
Clinical characteristics
Pancreatic heterotopia can be found in two clinical set
tings in the stomach. the first presentation, only rarely Figure 8 | A pancreatic heterotopia. a | endoscopic view showing a pyloric channel
seen endoscopically as a polyp, consists of small, sub polyp with a central dimple, which may be a draining pancreatic duct. Although
mucosal nodules (single or multiple, usually containing considered typical, this endoscopic appearance is by no means the most common.
only a few glands) of pancreatic tissue at the cardio Most pancreatic heterotopias are seen as small, smooth nodules lined by normal
gastric mucosa. b | Histological features of a nodule of pancreatic acinar tissue
esophageal junction; this finding is known as pancre
(limited by converging black arrows) completely surrounded by normal oxyntic
atic metaplasia, although whether it represents real mucosa. This is the most common microscopic appearance of pancreatic
metaplasia or heterotopia is unclear. this condition is heterotopia in the stomach, with neither ducts nor islets readily visible.
found in 5–15% of individuals who undergo endoscopy
for GerD and have a biopsy specimen taken from the
esophageal junction. in some studies, pancreatic meta the overwhelming majority of these specimens con
plasia at the cardioesophageal junction has been related sisted of normal or inflamed gastric mucosa. mucosal
to inflammation at the gastroesophageal junction. the folds, edema of the lamina propria, foveolar hyperplasia,
significance of this condition is unclear, but no indica and prominent lymphoid follicles might have the endo
tion that pancreatic metaplasia has neoplastic potential scopic appearance of a small polyp. the practice, now
has been found.78,79 routine in many centers, to attach an endoscopic picture
the other type of pancreatic heterotopia is usually or a detailed description of the lesion to the pathol
discovered as a submucosal lesion in the antral and ogy requisition is crucial to formulation of an informed
prepyloric regions of the stomach, sometimes with a report. For example, if endoscopy shows a smooth,
central dimple if a duct is present (Figure 8a). this type round antral nodule and the biopsy specimen reveals
is uncommon; it represents <1% of all gastric polyps.80 a perfectly normal mucosa, a sensible pathologist will
these lesions are solitary and composed mostly of acinar add a comment to suggest that the biopsy specimen may
tissue, often with ducts and seldom with islet cells. the not be representative of the lesion, and a submucosal
histology resembles normal pancreatic tissue. as is lesion may not have been sampled. if a malignant
the case with all submucosal lesions, they are easily missed looking, necrotic ulcerated lesion is seen endoscopi
in superficial biopsies (Figure 8b). the gastric mucosa cally, but the biopsy specimen shows only dysplastic,
that surrounds these lesions is usually unremarkable. but not invasive, epithelium, the pathology report
should clearly state that a repeat biopsy is necessary.
Management Gastroenterologists who routinely receive diag noses
Pancreatic heterotopia is a benign and usually asymptom of polypoid mucosa, mild hyperplastic features, and
atic lesion; thus, no therapy is warranted.80 symptomatic similar vacuous expressions should suspect that their
lesions (large enough to cause gastricoutlet obstruc pathologist is trying to appease them with a diagnosis
tion) are rare, and can be treated by resection.81 Ductal that fits the endoscopy. a frank conversation with the
adenocarcinomas, isletcell tumors, and pancreatitis pathologist and a few sessions at the microscope could
that arises in heterotopic pancreatic tissue have been go a long way to improve the specificity of diagnoses
reported, but the rarity of such occurrences suggests that and, ultimately, care of patients.
neither surgical excision nor endoscopic surveillance
are warranted.82,83 Conclusions
although no precise epidemiologic data exist, gastric
When a polyp is not a polyp polyps are common, and most often fall into the cate
in our 2009 series,10 16.1% of 7,925 gastric biopsy speci gories of fundicgland, hyperplastic, and adenomatous
mens identified endoscopically as a polyp or nodule had polyps. However, an impressive variety of gastric lesions
no histopathological features that could meet the diag might present as a polyp, and understanding the need
nostic criteria of one of the recognized gastric polyps. to obtain a biopsy specimen from the gastric mucosa
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 339
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
adjacent to a lesion is critical for a cohesive pathological Review criteria
diagnosis. although polyps are occasionally the cause
The MeDLiNe and PubMed databases were searched in
of symptoms that require endoscopic investigation,
October 2008 for english-language articles. The terms
they are often a marker of underlying gastritis that may “polyp”, “fundic-gland polyp”, “hyperplastic polyp”,
require diagnosis and treatment. appropriate surveil “adenoma”, “gastrointestinal stromal tumor”, “polyposis”,
lance proto cols, detailed above, exist for polyps with “pancreatic heterotopia”, “xanthoma”, “inflammatory
a known neoplastic risk, and the asGe surveillance fibroid” and “carcinoid” were combined with “stomach”
recommendations for polyps and polyposis syndromes and “gastric” to locate articles. reference lists were
checked for additional relevant papers.
are also available online.84
1. Park, D. Y. & Lauwers, G. Y. Gastric polyps: 17. raghunath, A. s. et al. review article: the long- hyperplastic gastric polyps. Am. J.
classification and management. Arch. Pathol. term use of proton-pump inhibitors. Aliment. Gastroenterol. 88, 1916–1919 (1993).
Lab. Med. 132, 633–640 (2008). Pharmacol. Ther. 22 (suppl. 1), 55–63 (2005). 34. Nogueira, A. M. et al. Microsatellite instability in
2. Ming, s. C. The classification and significance 18. Declich, P. et al. Fundic gland polyps and PPi: hyperplastic and adenomatous polyps of the
of gastric polyps. Monogr. Pathol. 18, 149–175 the Mozart effect of gastrointestinal stomach. Cancer 86, 1649–1656 (1999).
(1977). pathology? Pol. J. Pathol. 57, 181–182 (2006). 35. Murakami, K. et al. p53, but not c‑Ki‑ras,
3. stolte, M. Clinical consequences of the 19. vieth, M. & stolte, M. Fundic gland polyps are mutation and down-regulation of p21wAF1/
endoscopic diagnosis of gastric polyps. not induced by proton pump inhibitor therapy. CiP1 and cyclin D1 are associated with
Endoscopy 27, 32–37 (1995). Am. J. Clin. Pathol. 116, 716–720 (2001). malignant transformation in gastric hyperplastic
4. stolte, M. et al. Frequency, location, and age 20. Abraham, s. C. et al. sporadic fundic gland polyps. Am. J. Clin. Pathol. 115, 224–234
and sex distribution of various types of gastric polyps with epithelial dysplasia: evidence for (2001).
polyp. Endoscopy 26, 659–665 (1994). preferential targeting for mutations in the 36. Yao, T. et al. Malignant transformation of gastric
5. Archimandritis, A. et al. Gastric epithelial adenomatous polyposis coli gene. Am. J. hyperplastic polyps: alteration of phenotypes,
polyps: a retrospective endoscopic study of Pathol. 161, 1735–1742 (2002). proliferative activity, and p53 expression. Hum.
12974 symptomatic patients. Ital. J. 21. Abraham, s. C. et al. sporadic fundic gland Pathol. 33, 1016–1022 (2002).
Gastroenterol. 28, 387–390 (1996). polyps: common gastric polyps arising through 37. Hattori, T. Morphological range of hyperplastic
6. Morais, D. J. et al. Gastric polyps: activating mutations in the β-catenin gene. Am. polyps and carcinomas arising in hyperplastic
a retrospective analysis of 26,000 digestive J. Pathol. 158, 1005–1010 (2001). polyps of the stomach. J. Clin. Pathol. 38,
endoscopies. Arq. Gastroenterol. 44, 14–17 22. Torbenson, M. et al. sporadic fundic gland 622–630 (1985).
(2007). polyposis: a clinical, histological, and 38. Zea-iriarte, w. L. et al. Carcinoma in gastric
7. Nakamura, T. & Nakano, G. Histopathological molecular analysis. Mod. Pathol. 15, 718–723 hyperplastic polyps. A phenotypic study. Dig. Dis.
classification and malignant change in gastric (2002). Sci. 41, 377–386 (1996).
polyps. J. Clin. Pathol. 38, 754–764 (1985). 23. Declich, P. et al. Fundic gland polyps: a not so 39. Yoshihara, M. et al. Correlation of ratio of serum
8. Farinati, F. et al. early and advanced gastric innocuous entity worth a careful evaluation. pepsinogen i and ii with prevalence of gastric
cancer in the follow-up of moderate and severe Am. J. Gastroenterol. 93, 2641 (1998). cancer and adenoma in Japanese subjects. Am.
gastric dysplasia patients. A prospective study. 24. Dirschmid, K. et al. why is the hyperplastic J. Gastroenterol. 93, 1090–1096 (1998).
i. G. G. e. D.—-interdisciplinary Group on polyp a marker for the precancerous condition 40. Laxen, F. et al. Gastric polyps; their
Gastric epithelial Dysplasia. Endoscopy 25, of the gastric mucosa? Virchows Arch. 448, morphological and endoscopical characteristics
261–264 (1993). 80–84 (2006). and relation to gastric carcinoma. Acta Pathol.
9. Lauwers, G. Y. & srivastava, A. Gastric 25. Malaty, H. M. epidemiology of Helicobacter Microbiol. Immunol. Scand. [A]. 90, 221–228
preneoplastic lesions and epithelial dysplasia. pylori infection. Best Pract. Res. Clin. (1982).
Gastroenterol. Clin. North Am. 36, 813–829 Gastroenterol. 21, 205–214 (2007). 41. Abraham, s. C. et al. Genetic alterations in
(2007). 26. Abraham, s. C. et al. Hyperplastic polyps of the gastric adenomas of intestinal and foveolar
10. Carmack, s. w. et al. The current spectrum of stomach: associations with histologic patterns phenotypes. Mod. Pathol. 16, 786–795 (2003).
gastric polyps: a one-year national study of over of gastritis and gastric atrophy. Am. J. Surg. 42. Hirota, w. K. et al. AsGe guideline: the role of
120,000 patients. Am. J. Gastroenterol. (in Pathol. 25, 500–507 (2001). endoscopy in the surveillance of premalignant
press). 27. Cerwenka, H. et al. Pyloric obstruction caused conditions of the upper Gi tract. Gastrointest.
11. Bertoni, G. et al. Dysplastic changes in gastric by prolapse of a hyperplastic gastric polyp. Endosc. 63, 570–580 (2006).
fundic gland polyps of patients with familial Hepatogastroenterology 49, 958–960 (2002). 43. Dunlop, M. G. Guidance on gastrointestinal
adenomatous polyposis. Ital. J. Gastroenterol. 28. Chen, H. w. et al. Gastric outlet obstruction surveillance for hereditary non-polyposis
Hepatol. 31, 192–197 (1999). due to giant hyperplastic gastric polyps. colorectal cancer, familial adenomatous
12. Bianchi, L. K. et al. Fundic gland polyp J. Formos. Med. Assoc. 104, 852–855 (2005). polypolis, juvenile polyposis, and Peutz–Jeghers
dysplasia is common in familial adenomatous 29. Dixon, M. F. et al. reflux gastritis: syndrome. Gut 51 (suppl. 5), v21–v27 (2002).
polyposis. Clin. Gastroenterol. Hepatol. 6, distinct histopathological entity? J. Clin. Pathol. 44. Hizawa, K. et al. Juvenile polyposis of the
180–185 (2008). 39, 524–530 (1986). stomach: clinicopathological features and its
13. Attard, T. M. et al. Multicenter experience with 30. Genta, r. M. Differential diagnosis of reactive malignant potential. J. Clin. Pathol. 50, 771–774
upper gastrointestinal polyps in pediatric gastropathy. Semin. Diagn. Pathol. 22, (1997).
patients with familial adenomatous polyposis. 273–283 (2005). 45. Johnson, G. K. et al. Cronkite–Canada
Am. J. Gastroenterol. 99, 681–686 (2004). 31. Ljubicic, N. et al. The effect of eradicating syndrome: gastrointestinal pathophysiology and
14. Fossmark, r. et al. serum gastrin and Helicobacter pylori infection on the course of morphology. Gastroenterology 63, 140–152
chromogranin A levels in patients with fundic adenomatous and hyperplastic gastric polyps. (1972).
gland polyps caused by long-term proton-pump Eur. J. Gastroenterol. Hepatol. 11, 727–730 46. Hizawa, K. et al. Gastrointestinal manifestations
inhibition. Scand. J. Gastroenterol. 43, 1–5 (1999). of Cowden’s disease. report of four cases.
(2007). 32. Ohkusa, T. et al. Disappearance of hyperplastic J. Clin. Gastroenterol. 18, 13–18 (1994).
15. Kim, J. s. et al. spontaneous resolution of polyps in the stomach after eradication of 47. Jagelman, D. G. et al. Upper gastrointestinal
multiple fundic gland polyps after cessation Helicobacter pylori. A randomized, clinical trial. cancer in familial adenomatous polyposis.
of treatment with omeprazole. Korean J. Ann. Intern. Med. 129, 712–715 (1998). Lancet 1, 1149–1151 (1988).
Gastroenterol. 51, 305–308 (2008). 33. Lauwers, G. Y. et al. p53 expression in 48. Offerhaus, G. J. et al. The risk of upper
16. el-Zimaity, H. M. et al. Fundic gland polyps precancerous gastric lesions: gastrointestinal cancer in familial adenomatous
developing during omeprazole therapy. Am. J. an immunohistochemical study of PAb 1801 polyposis. Gastroenterology 102, 1980–1982
Gastroenterol. 92, 1858–1860 (1997). monoclonal antibody on adenomatous and (1992).
340 | JUNE 2009 | volUmE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
reviews
49. Giardiello, F. M. et al. very high risk of cancer in mesylate era-—a population-based study in 75. schindl, M. et al. Treatment of gastric
familial Peutz–Jeghers syndrome. western sweden. Cancer 103, 821–829 (2005). neuroendocrine tumors: the necessity of a type-
Gastroenterology 119, 1447–1453 (2000). 63. Kawanowa, K. et al. High incidence of microscopic adapted treatment. Arch. Surg. 136, 49–54
50. McGrath, D. r. & spigelman, A. D. Preventive gastrointestinal stromal tumors in the stomach. (2001).
measures in Peutz–Jeghers syndrome. Fam. Hum. Pathol. 37, 1527–1535 (2006). 76. Yi, s. Y. Dyslipidemia and H. pylori in gastric
Cancer 1, 121–125 (2001). 64. DeMatteo, r. P. et al. Two hundred gastrointestinal xanthomatosis. World J. Gastroenterol. 13,
51. Giardiello, F. M. & Trimbath, J. D. Peutz–Jeghers stromal tumors: recurrence patterns and 4598–4601 (2007).
syndrome and management recommendations. prognostic factors for survival. Ann. Surg. 231, 77. Lin, P. Y. et al. Gastric xanthelasma in
Clin. Gastroenterol. Hepatol. 4, 408–415 (2006). 51–58 (2000). hyperplastic gastric polyposis. Arch. Pathol. Lab.
52. Howe, J. r. et al. The risk of gastrointestinal 65. Demetri, G. D. et al. NCCN Task Force report: Med. 113, 428–430 (1989).
carcinoma in familial juvenile polyposis. Ann. management of patients with gastrointestinal 78. el-serag, H. B. et al. Prevalence and
Surg. Oncol. 5, 751–756 (1998). stromal tumor (GisT)-—update of the NCCN determinants of histological abnormalities of
53. ward, e. M. & wolfsen, H. C. Pharmacological clinical practice guidelines. J. Natl Compr. Canc. the gastric cardia in volunteers. Scand. J.
management of Cronkhite–Canada syndrome. Netw. 5 (suppl. 2), 1–9 (2007). Gastroenterol. 42, 1158–1166 (2007).
Expert Opin. Pharmacother. 4, 385–389 (2003). 66. Hueman, M. T. & schulick, r. D. Management of 79. Polkowski, w. et al. intestinal and pancreatic
54. wirtzfeld, D. A. et al. Hamartomatous polyposis gastrointestinal stromal tumors. Surg. Clin. North metaplasia at the esophagogastric junction in
syndromes: molecular genetics, neoplastic risk, Am. 88, 599–614 (2008). patients without Barrett’s esophagus. Am. J.
and surveillance recommendations. Ann. Surg. 67. Nilsson, B. et al. Adjuvant imatinib treatment Gastroenterol. 95, 617–625 (2000).
Oncol. 8, 319–327 (2001). improves recurrence-free survival in patients with 80. Christodoulidis, G. et al. Heterotopic pancreas in
55. Hasegawa, T. et al. CD34 expression by high-risk gastrointestinal stromal tumours (GisT). the stomach: a case report and literature review.
inflammatory fibroid polyps of the stomach. Br. J. Cancer 96, 1656–1658 (2007). World J. Gastroenterol. 13, 6098–6100 (2007).
Mod. Pathol. 10, 451–456 (1997). 68. Gilligan, C. J. et al. Gastric carcinoid tumors: 81. Ormarsson, O. T. et al. Diagnosis and treatment
56. Puri, A. s. et al. Giant inflammatory fibroid polyp the biology and therapy of an enigmatic and of gastric heterotopic pancreas. World J. Surg.
of stomach causing massive upper controversial lesion. Am. J. Gastroenterol. 90, 30, 1682–1689 (2006).
gastrointestinal bleeding. Indian J. Gastroenterol. 338–352 (1995). 82. Ayantunde, A. A. et al. symptomatic pyloric
10, 23–24 (1991). 69. Kloppel, G. et al. The gastroenteropancreatic pancreatic heterotopia: report of three cases
57. Allibone, r. O. et al. Multiple and recurrent neuroendocrine cell system and its tumors: and review of the literature. Med. Sci. Monit. 12,
inflammatory fibroid polyps in a Devon family the wHO classification. Ann. NY Acad. Sci. 1014, Cs49–Cs52 (2006).
(‘Devon polyposis syndrome’): an update. Gut 13–27 (2004). 83. Chetty, r. & weinreb, i. Gastric neuroendocrine
33, 1004–1005 (1992). 70. Kloppel, G. et al. Pathology and nomenclature of carcinoma arising from heterotopic pancreatic
58. Pantanowitz, L. et al. inflammatory fibroid polyps human gastrointestinal neuroendocrine tissue. J. Clin. Pathol. 57, 314–317 (2004).
of the gastrointestinal tract: evidence for a (carcinoid) tumors and related lesions. World J. 84. AsGe guideline: the role of endoscopy in the
dendritic cell origin. Am. J. Surg. Pathol. 28, Surg. 20, 132–141 (1996). surveillance of premalignant conditions of the
107–114 (2004). 71. rindi, G. et al. eCL cell tumor and poorly upper Gi tract. National Guidelines
59. schildhaus, H. U. et al. inflammatory fibroid differentiated endocrine carcinoma of the Clearinghouse [online] http://www.guideline.
polyps harbour mutations in the platelet-derived stomach: prognostic evaluation by pathological gov/summary/summary.aspx?doc_id=9306
growth factor receptor α (PDGFrA) gene. analysis. Gastroenterology 116, 532–542 (2009).
J. Pathol. 216, 176–182 (2008). (1999).
60. Paikos, D. et al. inflammatory fibroid polyp or 72. rindi, G. et al. Gastric carcinoids and acknowledgments
vanek’s tumour. Dig. Surg. 24, 231–233 (2007). neuroendocrine carcinomas: pathogenesis, we would like to thank Dr A. Horiuchi, showa inan
61. Miettinen, M. & Lasota, J. Gastrointestinal pathology, and behavior. World J. Surg. 20, General Hospital, Komagane, Japan for providing the
stromal tumors-—definition, clinical, histological, 168–172 (1996). endoscopic photographs of a gastric adenoma
immunohistochemical, and molecular genetic 73. Borch, K. et al. Gastric carcinoids: (Figure 3a) and a gastric carcinoid (Figure 6a).
features and differential diagnosis. Virchows biologic behavior and prognosis after Charles P. vega, University of California, irvine, CA, is
Arch. 438, 1–12 (2001). differentiated treatment in relation to type. Ann. the author of and is solely responsible for the content
62. Nilsson, B. et al. Gastrointestinal stromal Surg. 242, 64–73 (2005). of the learning objectives, questions and answers of
tumors: the incidence, prevalence, clinical 74. Modlin, i. M. et al. Gastric carcinoids. The Yale the Medscape-accredited continuing medical
course, and prognostication in the preimatinib experience. Arch. Surg. 130, 250–255 (1995). education activity associated with this article.
nature reviews | gastroenterology & hepatology volume 6 | June 2009 | 341
© 2009 Macmillan Publishers Limited. All rights reserved
You might also like
- Clinical Guidelines Secondary Prevention of Gastric CancerDocument1 pageClinical Guidelines Secondary Prevention of Gastric Cancerhenrique.uouNo ratings yet
- Gastritis and Carditis: University of British Columbia, Vancouver, British Columbia, CanadaDocument17 pagesGastritis and Carditis: University of British Columbia, Vancouver, British Columbia, CanadaJose SirittNo ratings yet
- What S Hidden Under The Gastric Intestinal Metaplasia Diffuse Type Adenocarcinoma Discovered by Targeted Biopsies A Case ReportDocument4 pagesWhat S Hidden Under The Gastric Intestinal Metaplasia Diffuse Type Adenocarcinoma Discovered by Targeted Biopsies A Case ReportHerald Scholarly Open AccessNo ratings yet
- Autoimmune Atrophic Gastritis CurrentDocument9 pagesAutoimmune Atrophic Gastritis CurrentXiomara CuadrosNo ratings yet
- Use of Endoscopic Assessment of Gastric Atrophy For Gastric Cancer Risk Stratification To Reduce The Need For Gastric MappingDocument7 pagesUse of Endoscopic Assessment of Gastric Atrophy For Gastric Cancer Risk Stratification To Reduce The Need For Gastric MappingVanessa BecerraNo ratings yet
- CarcinogénesisDocument14 pagesCarcinogénesisLuis Adolfo BermudezNo ratings yet
- Gastric Hamartomatous PolypsDocument8 pagesGastric Hamartomatous Polypscc vereNo ratings yet
- DCR 2016 Constipation, Evaluation and Management ofDocument14 pagesDCR 2016 Constipation, Evaluation and Management ofrisewfNo ratings yet
- Gastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFDocument938 pagesGastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFRaluca MărgulescuNo ratings yet
- DiverticularDiseaseoftheColon PDFDocument12 pagesDiverticularDiseaseoftheColon PDFAdrian MucileanuNo ratings yet
- KJG074 01 04 PDFDocument13 pagesKJG074 01 04 PDFNovita AfsariNo ratings yet
- ACVIM Consensus Statement On Pancreatitis in CatsDocument21 pagesACVIM Consensus Statement On Pancreatitis in CatswilverNo ratings yet
- 2020 - Diet and Gastric CADocument5 pages2020 - Diet and Gastric CAPatricia Peñaflor GrimaldoNo ratings yet
- 2010 Endoscopic, Biopsy & Logic Guidelines For The Evaluation of Gi Inflammation in Companion AnimalsDocument17 pages2010 Endoscopic, Biopsy & Logic Guidelines For The Evaluation of Gi Inflammation in Companion AnimalsRachel JohnsonNo ratings yet
- Disfagia 222 PDFDocument11 pagesDisfagia 222 PDFSteven WilliamNo ratings yet
- Histopatologia Enf IntestinalDocument7 pagesHistopatologia Enf IntestinalmariaNo ratings yet
- Annals of Gastroent Surgery - 2023 - Iwatsuki - The Comprehensive ReviewDocument8 pagesAnnals of Gastroent Surgery - 2023 - Iwatsuki - The Comprehensive ReviewSCJUBv Chirurgie INo ratings yet
- Dickson 1989Document7 pagesDickson 1989Necesito esta cuentaNo ratings yet
- Functional Dyspepsia: Review ArticleDocument11 pagesFunctional Dyspepsia: Review Articlejenny puentesNo ratings yet
- OLGA Staging For GastritisDocument9 pagesOLGA Staging For GastritisAndrea AlesandraNo ratings yet
- Gastrojejunostomy For Gastric Outlet Obstruction in Patients With Gastric CarcinomaDocument4 pagesGastrojejunostomy For Gastric Outlet Obstruction in Patients With Gastric CarcinomacindyNo ratings yet
- 2016 Histo Ampullary CarcinomaDocument11 pages2016 Histo Ampullary CarcinomamaomaochongNo ratings yet
- Peptic: Treatment DiseaseDocument8 pagesPeptic: Treatment DiseaseClaudia CorjăuceanuNo ratings yet
- Gastric Precancerous Process in A High Risk Population Cohort Followup PELAYO CORREADocument5 pagesGastric Precancerous Process in A High Risk Population Cohort Followup PELAYO CORREAOscar VicenteNo ratings yet
- Changes in Gastric Mucosal Microbiota in Gastric Carcinogenesis: A Systematic Review ProtocolDocument10 pagesChanges in Gastric Mucosal Microbiota in Gastric Carcinogenesis: A Systematic Review ProtocolwulanesterNo ratings yet
- Sampling and Reporting of Inflammatory Bowel DiseaseDocument12 pagesSampling and Reporting of Inflammatory Bowel DiseaseDiego Fernando Ortiz TenorioNo ratings yet
- 1 s2.0 S0140673623009662 MainDocument14 pages1 s2.0 S0140673623009662 MainKesia MaldonadoNo ratings yet
- Guedeline For The Investigation of Chronic DiarrhoeaDocument16 pagesGuedeline For The Investigation of Chronic DiarrhoeanaryNo ratings yet
- Gastric Adenocarcinoma of The Fundic Gland TypeDocument13 pagesGastric Adenocarcinoma of The Fundic Gland TypeMaspNo ratings yet
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 pagesPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesNo ratings yet
- Gastritis - Etiology and Diagnosis - UpToDateDocument8 pagesGastritis - Etiology and Diagnosis - UpToDateMatheus AzevedoNo ratings yet
- Molecular Characterization of The Human Stomach Microbiota in Gastric Cancer PatientsDocument11 pagesMolecular Characterization of The Human Stomach Microbiota in Gastric Cancer PatientsNita SofianaNo ratings yet
- A Clinical Study of Gastric Outlet Obstruction in Adults''Document19 pagesA Clinical Study of Gastric Outlet Obstruction in Adults''safasayedNo ratings yet
- Bowel Preparation For Pediatric Colonoscopy AnakDocument8 pagesBowel Preparation For Pediatric Colonoscopy AnakrantaikarbonNo ratings yet
- Example 3Document8 pagesExample 3โสภาพรรณวดี รวีวารNo ratings yet
- Gut Microbiota-Derived Epigenetic Alterations During Onset of DiseasesDocument11 pagesGut Microbiota-Derived Epigenetic Alterations During Onset of DiseasesDiamondChuNo ratings yet
- 1 s2.0 S2255534X21000876 MainDocument16 pages1 s2.0 S2255534X21000876 MaintassneemosammaNo ratings yet
- The Surgical Management of Necrotizing Enterocolitis - July 2018Document4 pagesThe Surgical Management of Necrotizing Enterocolitis - July 2018Hengky TanNo ratings yet
- The American Society of Colon and Rectal Surgeons.6Document15 pagesThe American Society of Colon and Rectal Surgeons.6Emanuella CirinoNo ratings yet
- En - 0120 9957 RCG 32 03 00258Document10 pagesEn - 0120 9957 RCG 32 03 00258gvstbndyhkNo ratings yet
- Gastritis Bahasa InggrisDocument7 pagesGastritis Bahasa InggrisNieq Cutex CelaluingindimandjaNo ratings yet
- Current Concepts in Gastric Signet Ring Cell CarcinomaDocument7 pagesCurrent Concepts in Gastric Signet Ring Cell CarcinomaalifaNo ratings yet
- Clinical Practice Recommendations For The Management of Bowel ObstructionDocument11 pagesClinical Practice Recommendations For The Management of Bowel ObstructionThiago GomesNo ratings yet
- Mouse Models For Gastric Cancer Matching Models ToDocument16 pagesMouse Models For Gastric Cancer Matching Models ToUtami DewiNo ratings yet
- Biomarkers in Barrett's Esophagus and Esophageal Adenocarcinoma: Predictors of Progression and PrognosisDocument13 pagesBiomarkers in Barrett's Esophagus and Esophageal Adenocarcinoma: Predictors of Progression and PrognosisCarlos HidalgoNo ratings yet
- Acquired Gastrointestinal Fistulas-Classification, Etiologies, and Imaging EvaluationDocument15 pagesAcquired Gastrointestinal Fistulas-Classification, Etiologies, and Imaging EvaluationAle LizárragaNo ratings yet
- Pathophysiology, Diagnosis, and Management of Chronic Intestinal Pseudo-ObstructionDocument13 pagesPathophysiology, Diagnosis, and Management of Chronic Intestinal Pseudo-ObstructionJosealberto ArenasNo ratings yet
- The Fear of Gastric Cancer in Patients With Dyspepsia: Challenge in Specialist Care GastroenterologyDocument8 pagesThe Fear of Gastric Cancer in Patients With Dyspepsia: Challenge in Specialist Care GastroenterologyAhana MukherjeeNo ratings yet
- 06 Surgical Strategies in Complex GastroschisisDocument7 pages06 Surgical Strategies in Complex GastroschisisLorena TorresNo ratings yet
- Approche DCDocument16 pagesApproche DCnaryNo ratings yet
- J of Gastro and Hepatol - 2013 - SchillerDocument20 pagesJ of Gastro and Hepatol - 2013 - Schillerzakiah11No ratings yet
- Bond - 2000 - Polyp Guideline Diagnosis, Treatment, and Surveillance For Patients With Colorectal Polyps PDFDocument11 pagesBond - 2000 - Polyp Guideline Diagnosis, Treatment, and Surveillance For Patients With Colorectal Polyps PDFflashjetNo ratings yet
- PepticDocument4 pagesPepticmosmoh_52No ratings yet
- DispepsiaDocument11 pagesDispepsiaPendikNo ratings yet
- Functional Gastrointestinal Disorders 2: SeriesDocument14 pagesFunctional Gastrointestinal Disorders 2: SeriesStephani Fontinelli LeonardiNo ratings yet
- American College of Gastroenterology Guideline On.36Document18 pagesAmerican College of Gastroenterology Guideline On.36Nona RahayaanNo ratings yet
- Biliary Atresia: A Multidisciplinary Approach To Diagnosis and ManagementDocument15 pagesBiliary Atresia: A Multidisciplinary Approach To Diagnosis and ManagementAnne Lorraine BringasNo ratings yet
- GI - Pathophysiology, Evaluation, and Treatment of BloatingDocument11 pagesGI - Pathophysiology, Evaluation, and Treatment of BloatingTriLightNo ratings yet
- Gastroenterology For General SurgeonsFrom EverandGastroenterology For General SurgeonsMatthias W. WichmannNo ratings yet
- Essential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookFrom EverandEssential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookNo ratings yet
- VAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogensDocument11 pagesVAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogenscc vereNo ratings yet
- Z. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)Document928 pagesZ. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)cc vereNo ratings yet
- The Nuctemeron of Apollonius of TyanaDocument9 pagesThe Nuctemeron of Apollonius of Tyanacc vereNo ratings yet
- Ox InflammationDocument15 pagesOx Inflammationcc vereNo ratings yet
- Autonomic Immune Vascular InteractionDocument9 pagesAutonomic Immune Vascular Interactioncc vereNo ratings yet
- Oxytocin and VasopressinDocument19 pagesOxytocin and Vasopressincc vereNo ratings yet
- Wake Sleep CycleDocument11 pagesWake Sleep Cyclecc vereNo ratings yet
- Heart-Brain AxisDocument15 pagesHeart-Brain Axiscc vereNo ratings yet
- Brain Immune InteractionsDocument12 pagesBrain Immune Interactionscc vereNo ratings yet
- Principles of Allostasis Optimal DesignDocument36 pagesPrinciples of Allostasis Optimal Designcc vereNo ratings yet
- Sensory Hepatic NervesDocument9 pagesSensory Hepatic Nervescc vereNo ratings yet
- Brain-Heart InteractionsDocument22 pagesBrain-Heart Interactionscc vereNo ratings yet
- Stress Final Text 2016Document11 pagesStress Final Text 2016cc vereNo ratings yet
- Salivary GlandDocument64 pagesSalivary GlandDanielicah Cruz100% (1)
- GI BleedDocument96 pagesGI Bleedjaish8904100% (2)
- Sessile Serrated Adenoma - Libre PathologyDocument5 pagesSessile Serrated Adenoma - Libre PathologyfadoNo ratings yet
- ORAL-PATH-QP.-2021 RguhsDocument22 pagesORAL-PATH-QP.-2021 RguhsgautNo ratings yet
- CH 19 Non-Neoplastic Diseases of Salivary GlandsDocument55 pagesCH 19 Non-Neoplastic Diseases of Salivary GlandsReem E.MNo ratings yet
- ICD For OncologyDocument337 pagesICD For OncologytphivuongNo ratings yet
- Colon Polyps: Types, Diagnosis, and Treatment Options - Kaizen Gastro CareDocument2 pagesColon Polyps: Types, Diagnosis, and Treatment Options - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- MBBS Pathology-High-Yield TopicsDocument8 pagesMBBS Pathology-High-Yield TopicsRohith ReddyNo ratings yet
- Aisha Tabassum EtalDocument4 pagesAisha Tabassum EtaleditorijmrhsNo ratings yet
- Kiran sapru-NEWDocument4 pagesKiran sapru-NEWEvelyn ChacónNo ratings yet
- Optic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiDocument54 pagesOptic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiMohammed Jazeel 2549No ratings yet
- Ebook PDF Diagnostic Histopathology of Tumors 2 Volume Set 5th Edition PDFDocument40 pagesEbook PDF Diagnostic Histopathology of Tumors 2 Volume Set 5th Edition PDFjoe.andes67297% (37)
- (PATHOLOGY) NeoplasiaDocument137 pages(PATHOLOGY) Neoplasiaten tazapNo ratings yet
- AdenomaDocument4 pagesAdenomaPark JiminNo ratings yet
- Renal NeoplasmDocument153 pagesRenal NeoplasmTHESSNAVARRO100% (2)
- Gallbladder PolypDocument28 pagesGallbladder PolypChristian LoyolaNo ratings yet
- Pathology Ple SamplexDocument5 pagesPathology Ple SamplexdawnparkNo ratings yet
- Orallesions ClassificationDocument18 pagesOrallesions ClassificationRaj ChauhanNo ratings yet
- Faculty of Medicine and Health Sciences Score Sheet For CASE Write-UpDocument30 pagesFaculty of Medicine and Health Sciences Score Sheet For CASE Write-UpJared Khoo Er HauNo ratings yet
- SurgeryDocument31 pagesSurgeryGayathiri SureshNo ratings yet
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Referat Pleomorphic AdenomaDocument6 pagesReferat Pleomorphic AdenomaAsrie Sukawatie PutrieNo ratings yet
- Thyroid: Cytopathology and Its Histopathological BasesDocument49 pagesThyroid: Cytopathology and Its Histopathological BasesYuli Setio Budi PrabowoNo ratings yet
- 2,4-Diaminoanisole and Its Salts: 1.1 Chemical and Physical DataDocument25 pages2,4-Diaminoanisole and Its Salts: 1.1 Chemical and Physical DatakhoachiNo ratings yet
- BMA Illustrated Medical Dictionary, 3rd Edition PDFDocument610 pagesBMA Illustrated Medical Dictionary, 3rd Edition PDFAdina Manolescu86% (7)
- Adenoma 2020Document11 pagesAdenoma 2020Residentes AudiologiaNo ratings yet
- Cysts of Pancreas RADIOLOGYDocument20 pagesCysts of Pancreas RADIOLOGYmhany12345No ratings yet
- AdenocarcinomaDocument12 pagesAdenocarcinomaFeb LaoNo ratings yet
- SURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSDocument16 pagesSURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSBcBaba 007100% (1)
- Brain Tumors - Classifications, Symptoms, Diagnosis and TreatmentsDocument10 pagesBrain Tumors - Classifications, Symptoms, Diagnosis and TreatmentsshamimNo ratings yet