You might also like
- Ureteral Stones PtguideDocument11 pagesUreteral Stones Ptguidehanav90No ratings yet
- Litho Trips yDocument12 pagesLitho Trips yJasmine KaurNo ratings yet
- Kidney Stones: Jenny ZhaDocument16 pagesKidney Stones: Jenny ZhaJenny ZhaNo ratings yet
- Kidney Stone Owner's Manual v2Document12 pagesKidney Stone Owner's Manual v2Martin HaynesNo ratings yet
- LithotripsyDocument8 pagesLithotripsyITs MENo ratings yet
- Kidney Stone (About, Types and Treatment) - WhatsMedi Content ResearchhDocument4 pagesKidney Stone (About, Types and Treatment) - WhatsMedi Content ResearchhSiddharth ChoudheryNo ratings yet
- Reference Summary: X-Plain Lithotripsy - ESWLDocument6 pagesReference Summary: X-Plain Lithotripsy - ESWLFernanda PutriNo ratings yet
- Medico SurgicalDocument3 pagesMedico Surgicaljibson2354No ratings yet
- Kidney Stones: How To Treat Kidney Stones: How To Prevent Kidney StonesFrom EverandKidney Stones: How To Treat Kidney Stones: How To Prevent Kidney StonesRating: 5 out of 5 stars5/5 (1)
- Eswl 1Document33 pagesEswl 1G Vignesh GvsNo ratings yet
- a122010-0062021Document12 pagesa122010-0062021April RahmawatiNo ratings yet
- Lab KikneyDocument3 pagesLab KikneyAsma NaseemNo ratings yet
- University College London Hospitals: Ureteroscopy/UreterorenosDocument20 pagesUniversity College London Hospitals: Ureteroscopy/UreterorenosrakaNo ratings yet
- Extracorporeal Shock Wave Lithotripsy (ESWL (Document31 pagesExtracorporeal Shock Wave Lithotripsy (ESWL (emirilejlaNo ratings yet
- Kidney StonesDocument11 pagesKidney StonesNader Smadi100% (1)
- Symptoms: Kidney StonesDocument5 pagesSymptoms: Kidney StonesLucía Flores FaríasNo ratings yet
- UrolithiasisDocument7 pagesUrolithiasismariaNo ratings yet
- Spyglass PDFDocument4 pagesSpyglass PDFAnonymous DwQYfajfPvNo ratings yet
- Extracorporeal Shock Wave Lithotripsy (Eswl) : Patient InformationDocument2 pagesExtracorporeal Shock Wave Lithotripsy (Eswl) : Patient InformationFernanda PutriNo ratings yet
- 51 Tips For Dealing With Kidney StonesDocument16 pages51 Tips For Dealing With Kidney StonesFeenyxNo ratings yet
- Bladder Stone Treatment and CausesDocument13 pagesBladder Stone Treatment and CausesSher KhanNo ratings yet
- Diagnosis: Small Stones With Minimal SymptomsDocument5 pagesDiagnosis: Small Stones With Minimal SymptomsKatte VillenasNo ratings yet
- Topic 9Document5 pagesTopic 989qqzp4yhkNo ratings yet
- Urology Notes 1Document43 pagesUrology Notes 1Shazaan NadeemNo ratings yet
- UrolithiasisDocument3 pagesUrolithiasisMaan NavaroNo ratings yet
- Kidney StonesDocument11 pagesKidney StonesclubsanatateNo ratings yet
- Kidney stones: causes, symptoms and treatmentDocument3 pagesKidney stones: causes, symptoms and treatmentSisti AninditaNo ratings yet
- Your Ureteric Stent: A Patient's GuideDocument2 pagesYour Ureteric Stent: A Patient's GuidenaughtychanduNo ratings yet
- NeprolithotomyDocument3 pagesNeprolithotomyjesse caballeroNo ratings yet
- CystolithiasisDocument7 pagesCystolithiasisRaul Nocete100% (1)
- Management of Ureteric StoneDocument4 pagesManagement of Ureteric StoneAung Ko HtetNo ratings yet
- Renal Stone and Renal FailureDocument14 pagesRenal Stone and Renal FailurereboNo ratings yet
- MF 3 2017 Sotosek Ahel Rubinic Smolic MarkicDocument7 pagesMF 3 2017 Sotosek Ahel Rubinic Smolic MarkicbololocovcNo ratings yet
- Nephrectomy: The Advantages of Laparoscopic Surgery IncludeDocument5 pagesNephrectomy: The Advantages of Laparoscopic Surgery IncludeLouie ParillaNo ratings yet
- URINARY SYSTEM - AssignmentDocument6 pagesURINARY SYSTEM - Assignment6tsqs5bcs4No ratings yet
- SurgeyDocument37 pagesSurgeyDr Anais AsimNo ratings yet
- Kidney StonesDocument17 pagesKidney Stonessv swamy100% (1)
- KIDNEY STONES - LetterDocument6 pagesKIDNEY STONES - LetterFloreleneNo ratings yet
- Batu GinjalDocument3 pagesBatu GinjalHerdy AdrianoNo ratings yet
- PCNL Consent FormDocument4 pagesPCNL Consent FormSaisabelaNo ratings yet
- Non-Surgical Treatment For Urinary Stones - Urinary Stones Treatment in IndiasDocument8 pagesNon-Surgical Treatment For Urinary Stones - Urinary Stones Treatment in IndiasindiacarezNo ratings yet
- Ureteroscopic Lithotripsy Patient InstructionsDocument6 pagesUreteroscopic Lithotripsy Patient InstructionsMohd SukriNo ratings yet
- Kidney Stones 1Document4 pagesKidney Stones 1mynksharma100% (1)
- UROLITHIASISDocument3 pagesUROLITHIASISgwynethntpNo ratings yet
- Renal StonesDocument12 pagesRenal StonesDamandeep KaurNo ratings yet
- KB 10Document5 pagesKB 10Reband AzadNo ratings yet
- Urostomy: A Guide to Understanding Urinary Diversion SurgeryDocument26 pagesUrostomy: A Guide to Understanding Urinary Diversion SurgeryPattia1980No ratings yet
- SAGES Gallbladder CBDDocument54 pagesSAGES Gallbladder CBDSAGESWeb100% (1)
- Surgical Procedure - Kidney StoneDocument1 pageSurgical Procedure - Kidney StoneRoschelle VillamarNo ratings yet
- Lithotripsy Brochure Tcm28-177886Document24 pagesLithotripsy Brochure Tcm28-177886Jobelle GuevarraNo ratings yet
- AMVS Ureteral Obstruction SUB 2018Document2 pagesAMVS Ureteral Obstruction SUB 2018Christiné PunctNo ratings yet
- What Is A Bone Scan?: Prostate CancerDocument4 pagesWhat Is A Bone Scan?: Prostate CancerThisanthi KayNo ratings yet
- Urinary Calculus Group 2Document26 pagesUrinary Calculus Group 2nayaashrrrNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- 333-Article Text-563-1-10-20180226Document9 pages333-Article Text-563-1-10-20180226No NameNo ratings yet
- CaseDocument7 pagesCaseAia JavierNo ratings yet
- Ultrasonography TheDocument3 pagesUltrasonography TheNor-aina Edding AbubakarNo ratings yet
- Nanotechnology PosterDocument5 pagesNanotechnology PosterFred JacksonNo ratings yet
- Refrigerators: Large Capacity Enviro-CentersDocument5 pagesRefrigerators: Large Capacity Enviro-CentersEng-Mugahed AlmansorNo ratings yet
- Centrifuge: University of Alkafeel Technical Laboratory Techniques Stage 1 Group A2 Rawan Odai AbbasDocument4 pagesCentrifuge: University of Alkafeel Technical Laboratory Techniques Stage 1 Group A2 Rawan Odai AbbasEng-Mugahed AlmansorNo ratings yet
- Large Capacity Laboratory Refrigerators: MPR-1410 MPR-1410R MPR-721 MPR-721RDocument6 pagesLarge Capacity Laboratory Refrigerators: MPR-1410 MPR-1410R MPR-721 MPR-721REng-Mugahed AlmansorNo ratings yet
- ALC Centrifuge ManualDocument27 pagesALC Centrifuge ManualEng-Mugahed AlmansorNo ratings yet
- CH 9Document9 pagesCH 9Jefferson SantanaNo ratings yet
- The Biomedical Engineering Handbook: Second EditionDocument13 pagesThe Biomedical Engineering Handbook: Second EditionEng-Mugahed AlmansorNo ratings yet
- 01 Product Overview & OperationDocument46 pages01 Product Overview & OperationEng-Mugahed AlmansorNo ratings yet
- Gambro Ak 200Document116 pagesGambro Ak 200jayramdeepak40% (5)
- The Biomedical Engineering Handbook: Second EditionDocument13 pagesThe Biomedical Engineering Handbook: Second EditionJefferson SantanaNo ratings yet
- Gambro Ak 200Document116 pagesGambro Ak 200jayramdeepak40% (5)
- Pco2 Po2Document7 pagesPco2 Po2ARIJIT DASNo ratings yet
- The Biomedical Engineering Handbook: Second EditionDocument8 pagesThe Biomedical Engineering Handbook: Second EditionEng-Mugahed AlmansorNo ratings yet
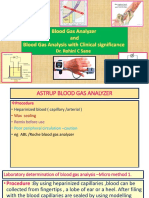
- Bloodgasanalyserbloodgasanalysiswithclinicalsignificance 160727131155 PDFDocument54 pagesBloodgasanalyserbloodgasanalysiswithclinicalsignificance 160727131155 PDFEng-Mugahed AlmansorNo ratings yet
- Bloodgasanalyserbloodgasanalysiswithclinicalsignificance 160727131155 PDFDocument54 pagesBloodgasanalyserbloodgasanalysiswithclinicalsignificance 160727131155 PDFEng-Mugahed AlmansorNo ratings yet
- Neumonia Por Aspiracion BookDocument232 pagesNeumonia Por Aspiracion BookRodrigo Navia ValenzuelaNo ratings yet
- Camping Recreational ActivityDocument5 pagesCamping Recreational ActivityGylle Marie PlazaNo ratings yet
- T2DM Office Visit ChecklistDocument2 pagesT2DM Office Visit Checklisthimura_gibsonNo ratings yet
- Vitamin NutritionDocument13 pagesVitamin NutritionSobita SharmaNo ratings yet
- Meda QantasDocument12 pagesMeda QantasAviasiNo ratings yet
- All About NailsDocument16 pagesAll About NailsJoel MarasiganNo ratings yet
- NADSS Training Iteya 2021Document27 pagesNADSS Training Iteya 2021abdilama13No ratings yet
- Type 2 Diabetes MellitusDocument1 pageType 2 Diabetes MellitusJúlia MeixnerNo ratings yet
- Aj CSF - Rhinorrhea - + - Nasal - Foreign - Body - + - Myiasis - + - ChoanalDocument63 pagesAj CSF - Rhinorrhea - + - Nasal - Foreign - Body - + - Myiasis - + - ChoanalTradigrade PukarNo ratings yet
- ASPS2021 InService SyllabusDocument414 pagesASPS2021 InService Syllabusreemali69No ratings yet
- P.E. & Health: Quarter 1 - Module 1: Self - Assessment Health - Related Fitness (HRF)Document30 pagesP.E. & Health: Quarter 1 - Module 1: Self - Assessment Health - Related Fitness (HRF)Rowena Chua Alvarez100% (1)
- High Yield Step 1 ImagesDocument65 pagesHigh Yield Step 1 Imagesaditya mishraNo ratings yet
- Bahasa Inggris Kel.2Document28 pagesBahasa Inggris Kel.2Listi PujiNo ratings yet
- Ethics On Consumers.Document7 pagesEthics On Consumers.Sujata KunduNo ratings yet
- Beta Blockers: ExampleDocument9 pagesBeta Blockers: ExampletiaraNo ratings yet
- Ehaa605 PDFDocument80 pagesEhaa605 PDFaspxxNo ratings yet
- HUMAN PHYSIOLOGY KEY FUNCTIONSDocument17 pagesHUMAN PHYSIOLOGY KEY FUNCTIONSplsssssNo ratings yet
- Parent HandbookDocument7 pagesParent Handbookapi-238446737No ratings yet
- Chapter 2Document24 pagesChapter 2Eden Marie FranciscoNo ratings yet
- Tetralogy of Fallot: Anatomic Variants and Their Impact On Surgical ManagementDocument9 pagesTetralogy of Fallot: Anatomic Variants and Their Impact On Surgical ManagementRoberto AmayaNo ratings yet
- Hidradenitis Suppurativa - A Disease Primer. Alexa B. Kimball, Gregor B.E. Jemec. 2017. Adis, ChamDocument59 pagesHidradenitis Suppurativa - A Disease Primer. Alexa B. Kimball, Gregor B.E. Jemec. 2017. Adis, ChammeliaNo ratings yet
- Scarlet Fever - Background, Pathophysiology, EtiologyDocument8 pagesScarlet Fever - Background, Pathophysiology, EtiologyPaskalia ChristinNo ratings yet
- TuberculosisDocument9 pagesTuberculosisIdasari DewiNo ratings yet
- 【医脉通】2021 EAST实践指南:横纹肌溶解症的管理Document9 pages【医脉通】2021 EAST实践指南:横纹肌溶解症的管理rd ytNo ratings yet
- Head To Toe AssessmentDocument2 pagesHead To Toe AssessmentAyucahyaNo ratings yet
- TATALAKSANA PROGNOSIS Cushing SyndromeDocument13 pagesTATALAKSANA PROGNOSIS Cushing SyndromeFirda RidhayantiNo ratings yet
- Guia Perioperatoria de CardioDocument115 pagesGuia Perioperatoria de Cardioxavi0725No ratings yet
- Wa482303 1698907992-4369872Document6 pagesWa482303 1698907992-4369872VN Machines Private LimitedNo ratings yet
- Cave Rescue ExerciseDocument3 pagesCave Rescue ExerciserajeshNo ratings yet
- Common Short Exam Cases in PediatricsDocument148 pagesCommon Short Exam Cases in PediatricsKoricho Mengistu100% (2)