You might also like
- Ardiac: Sudil Paudyal M.Sc. Mit (12) IOM, MMCDocument94 pagesArdiac: Sudil Paudyal M.Sc. Mit (12) IOM, MMCmirza alfariziNo ratings yet
- DR - Sakher-Alkhaderi: Consultant Radiologist AmcDocument50 pagesDR - Sakher-Alkhaderi: Consultant Radiologist AmcAswin Rajasekaran100% (1)
- Deteksi Penyakit Jantung Koroner Dengan MSCT 64 Slice: Franky J. Dimpudus, B.SC (Med - Imaging) (Curtin)Document17 pagesDeteksi Penyakit Jantung Koroner Dengan MSCT 64 Slice: Franky J. Dimpudus, B.SC (Med - Imaging) (Curtin)SyaraNo ratings yet
- Aortic, Renal, and Carotid CT Angiography: Matthew J. BudoffDocument13 pagesAortic, Renal, and Carotid CT Angiography: Matthew J. BudoffCarol ArtigasNo ratings yet
- CT Angiography of The Renal Arteries and Veins - Normal Anatomy and VariantsDocument7 pagesCT Angiography of The Renal Arteries and Veins - Normal Anatomy and VariantsthoiphamNo ratings yet
- Aortic DissectionDocument13 pagesAortic Dissectiondr IggyNo ratings yet
- 2-Dwita Gradien - 2 PDFDocument7 pages2-Dwita Gradien - 2 PDFTiffany CollinsNo ratings yet
- Coronary Circulatio1Document6 pagesCoronary Circulatio1merin sunilNo ratings yet
- BJR 83 194 PericardiumDocument12 pagesBJR 83 194 Pericardiumfranti76No ratings yet
- Multi-Modal CT Scanning in The Evaluation of Cerebrovascular Disease PatientsDocument18 pagesMulti-Modal CT Scanning in The Evaluation of Cerebrovascular Disease PatientsmicozaaaNo ratings yet
- Chapter 01 - Principles of Echocardiography - 1Document12 pagesChapter 01 - Principles of Echocardiography - 1maca_mike5723No ratings yet
- Cardiac Computed Tomography Technology PDFDocument73 pagesCardiac Computed Tomography Technology PDFRamona GhengheaNo ratings yet
- Adriaans2019 Article PredictiveImagingForThoracicAoDocument9 pagesAdriaans2019 Article PredictiveImagingForThoracicAohengkileonardNo ratings yet
- Carotid Artery Stenosis ImagingDocument10 pagesCarotid Artery Stenosis ImagingCristhian RuizNo ratings yet
- Coronaryangiography 180613180852Document64 pagesCoronaryangiography 180613180852Saud ShirwanNo ratings yet
- Coronaryangiography 180613180852Document64 pagesCoronaryangiography 180613180852Saud ShirwanNo ratings yet
- Carotid and Vertebral Ultrasonography - Dr. DanielDocument74 pagesCarotid and Vertebral Ultrasonography - Dr. DanielSuci Rahayu Evasha100% (1)
- Pi Is 0003497516313285Document3 pagesPi Is 0003497516313285Gordana PuzovicNo ratings yet
- Myocardial Revascularization: Margy P. Paredes Caballero 01180021022 Practice IIIDocument24 pagesMyocardial Revascularization: Margy P. Paredes Caballero 01180021022 Practice IIIapi-541444175No ratings yet
- Anatomía Del Seno Coronario y Su Importancia, Revisión Basada en La EvidenciaDocument3 pagesAnatomía Del Seno Coronario y Su Importancia, Revisión Basada en La EvidenciaCarlos GamezNo ratings yet
- Basic Cardiac ImagingDocument40 pagesBasic Cardiac ImagingSarah Sy-SantosNo ratings yet
- Dr. G.N. Prabhu Associate Professor Cardiothoracic Surgery SRM MCH & RCDocument60 pagesDr. G.N. Prabhu Associate Professor Cardiothoracic Surgery SRM MCH & RCNithya SekarNo ratings yet
- Heart Sound Sensing Through MEMS MicrophoneDocument12 pagesHeart Sound Sensing Through MEMS MicrophoneamarolimaNo ratings yet
- Coronary Revascularization: Margy P. Paredes Caballero 01180021022 Practice IIIDocument21 pagesCoronary Revascularization: Margy P. Paredes Caballero 01180021022 Practice IIIapi-541444175No ratings yet
- Vascular Imaging EquipmentsDocument50 pagesVascular Imaging EquipmentsRohit nikam0% (1)
- Aorta Referans AralıklarıDocument36 pagesAorta Referans AralıklarıALEX BORNo ratings yet
- Blood Supply of The HeartDocument5 pagesBlood Supply of The HeartMohammed EljackNo ratings yet
- Chest Part 3Document48 pagesChest Part 3rakshit09100% (1)
- Anatomy and Imaging of Coronary Artery Disease With Special Referance To CT Coronary AngiographyDocument125 pagesAnatomy and Imaging of Coronary Artery Disease With Special Referance To CT Coronary Angiographyﻣﻠﻚ عيسىNo ratings yet
- Primary Angioplasty in Anomalous Right Coronary Artery OriginatingDocument3 pagesPrimary Angioplasty in Anomalous Right Coronary Artery Originatingapi-560931483No ratings yet
- 1 s2.0 S2468644123001299 MainDocument6 pages1 s2.0 S2468644123001299 MainRonald QuezadaNo ratings yet
- 5 Min - Myocardial Strain AnalysisDocument26 pages5 Min - Myocardial Strain AnalysisAsim Kumar Biswas100% (1)
- Assessment of Left Ventricular Myocardial Diseases With Cardiac Computed TomographyDocument19 pagesAssessment of Left Ventricular Myocardial Diseases With Cardiac Computed Tomographysyifa auliaNo ratings yet
- Jead 024Document21 pagesJead 024wassim wassimNo ratings yet
- Anato IMAO BrainDocument220 pagesAnato IMAO BrainVilasecaNo ratings yet
- 5 Arta Al EditorDocument3 pages5 Arta Al EditorJuan José CabezasNo ratings yet
- 2d WMT 1Document4 pages2d WMT 1Nam LeNo ratings yet
- Bedah VaskulerDocument20 pagesBedah VaskulerArif WahyudiNo ratings yet
- Rido, Rudini - Disease of Aorta and Trauma To The AortaDocument114 pagesRido, Rudini - Disease of Aorta and Trauma To The AortaFikriYTNo ratings yet
- CT of The HeartDocument12 pagesCT of The HeartGil PerezNo ratings yet
- K 29 Sirkulasi Koroner - CVS K29Document16 pagesK 29 Sirkulasi Koroner - CVS K29Jane Andrea Christiano DjianzonieNo ratings yet
- The Radiology Assistant - Thoracic Aorta - The Acute Aortic SyndromeDocument13 pagesThe Radiology Assistant - Thoracic Aorta - The Acute Aortic SyndromeMitulsinh M RavaljiNo ratings yet
- Dissection Octobre 2019Document48 pagesDissection Octobre 2019ARMVOPNo ratings yet
- Lecture 6 Cardiovascular: Vascular System - The HemodynamicsDocument70 pagesLecture 6 Cardiovascular: Vascular System - The HemodynamicsAndreea ŞtefănescuNo ratings yet
- CH 21: Cardiovascular System - The Heart - : GoalsDocument21 pagesCH 21: Cardiovascular System - The Heart - : GoalsgopscharanNo ratings yet
- Acute Ischemic Stroke: How To Make A Brilliant Report: Poster No.: Congress: Type: AuthorsDocument63 pagesAcute Ischemic Stroke: How To Make A Brilliant Report: Poster No.: Congress: Type: AuthorsHugo Alberto C FNo ratings yet
- CH 21: Cardiovascular System - The HeartDocument21 pagesCH 21: Cardiovascular System - The HeartMadhuri DandamudiNo ratings yet
- AngiographyDocument3 pagesAngiographySai SridharNo ratings yet
- Jurnal RadiologiDocument26 pagesJurnal RadiologiItha Miftah TatuheyNo ratings yet
- Anatomia y Fisiologuia General Libro-851-900Document50 pagesAnatomia y Fisiologuia General Libro-851-900Felipe Aguirre CórdovaNo ratings yet
- Endovascular Repair of The Thoracic Aorta - UpToDateDocument48 pagesEndovascular Repair of The Thoracic Aorta - UpToDateAnca StanNo ratings yet
- Cardio ExpoDocument35 pagesCardio Expoapi-667225436No ratings yet
- Dca RahulDocument72 pagesDca RahulyuliaNo ratings yet
- Carotid Stenosis (Carotid Artery Disease)Document5 pagesCarotid Stenosis (Carotid Artery Disease)Pieter SteenkampNo ratings yet
- CTA CoronaryDocument39 pagesCTA CoronaryConsita VictoriaNo ratings yet
- 3D Speckle Tracking EchoDocument4 pages3D Speckle Tracking EchoDuchung TranNo ratings yet
- Sirkulasi KorenerDocument67 pagesSirkulasi KorenerAmalia Frantika WihardjoNo ratings yet
- Recent Innovations in Renal Vascular ImagingDocument16 pagesRecent Innovations in Renal Vascular ImagingHector Hernandez-SoriaNo ratings yet
- Nerve and Blood Supply of The Upper LimbDocument64 pagesNerve and Blood Supply of The Upper Limbenrico_aguila100% (5)
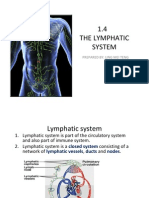
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNo ratings yet
- Assessment Management of Patients With Peripheral Vascular Disorders HypertensionDocument17 pagesAssessment Management of Patients With Peripheral Vascular Disorders HypertensionJhosita Flora LarocoNo ratings yet
- Clinmed 21 3 E275Document8 pagesClinmed 21 3 E275Carlos CoronaNo ratings yet
- EACVI TTE 250 Case ListDocument13 pagesEACVI TTE 250 Case ListBrînzoiu Olimpia50% (2)
- NCP Decreased Cardiac OutputDocument2 pagesNCP Decreased Cardiac OutputYamete KudasaiNo ratings yet
- Transport in Humans: Test Yourself 8.1 (Page 140)Document3 pagesTransport in Humans: Test Yourself 8.1 (Page 140)lee100% (3)
- Cardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarDocument29 pagesCardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarEka AriasyahNo ratings yet
- Effect of Temperature On FrogDocument2 pagesEffect of Temperature On FrogPrerna DubeyNo ratings yet
- Selim Mahmoud Abdel-Hakim: by Professor DRDocument27 pagesSelim Mahmoud Abdel-Hakim: by Professor DRAhmed TarekNo ratings yet
- Advanced EKG RefresherDocument181 pagesAdvanced EKG Refreshersimi100% (4)
- Anatomy and Physiology of Circle of WillisDocument23 pagesAnatomy and Physiology of Circle of WillisMohamed shukri elmiNo ratings yet
- Anatomy and Physiology of The HeartDocument21 pagesAnatomy and Physiology of The HeartNina OaipNo ratings yet
- Toate Bolile CardiovasculareDocument6 pagesToate Bolile CardiovasculareAnca CopreanNo ratings yet
- Case StudyDocument3 pagesCase StudyllulabyNo ratings yet
- NCM 106 Cardiac DrugsDocument111 pagesNCM 106 Cardiac DrugsKatie HolmesNo ratings yet
- Clonidine: Rahayu Mustika SariDocument20 pagesClonidine: Rahayu Mustika SarirahayuNo ratings yet
- Strokeaha 121 034436Document11 pagesStrokeaha 121 034436Matthew Czar TaonNo ratings yet
- Edexcel A Level Biology Key TermsDocument2 pagesEdexcel A Level Biology Key TermsShifa RahmanNo ratings yet
- Concept Map By: Debbie Cresta Capella University NURS-FPX6021: Biopsychosocial Concepts For Advanced Nursing Practice 1 Dr. Katie Hooven June 2, 2021Document3 pagesConcept Map By: Debbie Cresta Capella University NURS-FPX6021: Biopsychosocial Concepts For Advanced Nursing Practice 1 Dr. Katie Hooven June 2, 2021Debbie CrestaNo ratings yet
- Cardiac EmergenciesDocument26 pagesCardiac Emergenciespreet kaurNo ratings yet
- Key Points: Schwartz's Principles of Surgery Chapter 23. Arterial DiseaseDocument142 pagesKey Points: Schwartz's Principles of Surgery Chapter 23. Arterial DiseaseMohammad FareedNo ratings yet
- CARDIAC TUMORS Approach To ManagementDocument12 pagesCARDIAC TUMORS Approach To ManagementAnkit GulatiNo ratings yet
- Scrotum Anatomy and Scanning TechniqueDocument7 pagesScrotum Anatomy and Scanning TechniqueAnonymous wyF4yQZwZNo ratings yet
- Arb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirDocument40 pagesArb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirFidel Martua MarpaungNo ratings yet
- Test For Autonomic NeuropathyDocument31 pagesTest For Autonomic NeuropathysrinidhiNo ratings yet
- Cathlab Manual Coronary AngiographyDocument28 pagesCathlab Manual Coronary AngiographyNavojit Chowdhury100% (5)
- Neurology Clinical Cases PDFDocument219 pagesNeurology Clinical Cases PDFHandre PutraNo ratings yet
- Klasifikasi LimfomaDocument5 pagesKlasifikasi LimfomaBadlina Fitrianisa YulianingrumNo ratings yet
- Atherosclerosis and ArteriosclerosisDocument50 pagesAtherosclerosis and ArteriosclerosisApril Carter100% (1)