You might also like
- Small Animal Emergency and Critical Care Medicine - Kirby, Rebecca, Rudloff, Elke, Linklater, Drew PDFDocument249 pagesSmall Animal Emergency and Critical Care Medicine - Kirby, Rebecca, Rudloff, Elke, Linklater, Drew PDFSanjeev Choudhary100% (2)
- ATSP Booklet 2023Document26 pagesATSP Booklet 2023Savanthi Carmaline de SilvaNo ratings yet
- Pre & Post Operative CareDocument20 pagesPre & Post Operative CareBobby Faisyal Rakhman0% (1)
- Nursing Care Plans For Burned PatientDocument5 pagesNursing Care Plans For Burned PatientJunah Marie Rubinos Palarca85% (26)
- Burns in PaediatricDocument62 pagesBurns in PaediatricMusa yohana75% (4)
- UpToDate - Management Acute PancreatitisDocument36 pagesUpToDate - Management Acute PancreatitisCarmen Elena Plaisanu100% (3)
- Integumentary System Review - BurnsDocument52 pagesIntegumentary System Review - BurnsmikErlhNo ratings yet
- Committee On Trauma Presents: Thermal InjuriesDocument35 pagesCommittee On Trauma Presents: Thermal InjuriesAlfina Aulia RizkiNo ratings yet
- Committee On Trauma Presents: Therma L InjuriesDocument35 pagesCommittee On Trauma Presents: Therma L InjuriesJavar SodicNo ratings yet
- Presentation Postop CareDocument60 pagesPresentation Postop Caresiti syazanaNo ratings yet
- General Care of The Surgical PatientDocument25 pagesGeneral Care of The Surgical PatientWendy Jeng100% (1)
- Temperature Inside OR: Presented byDocument19 pagesTemperature Inside OR: Presented bydr_trialNo ratings yet
- Note nsc432 Mod5 E4fhzhwemo2iupeDocument45 pagesNote nsc432 Mod5 E4fhzhwemo2iupeBosede OjoNo ratings yet
- Burn Management by Tajuu Seid: Surgical WardDocument33 pagesBurn Management by Tajuu Seid: Surgical Wardelias adugnaNo ratings yet
- NCM 109 Common Health Problems in TodddlersDocument9 pagesNCM 109 Common Health Problems in TodddlersMantilla, Kristina Cassandra A.No ratings yet
- Post-Operative Care: DR - Tehreem Nasir MBBS, RMPDocument58 pagesPost-Operative Care: DR - Tehreem Nasir MBBS, RMPAhmed SaeedNo ratings yet
- Combutio 2019Document52 pagesCombutio 2019Dannish Alii0% (1)
- Management of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHADocument53 pagesManagement of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHAawesome0% (1)
- Trauma 1Document45 pagesTrauma 1Abdul HaiNo ratings yet
- Week 2-BurnDocument53 pagesWeek 2-BurnManal jNo ratings yet
- Emergency Nursing: By: Keverne Jhay P. ColasDocument61 pagesEmergency Nursing: By: Keverne Jhay P. ColasGaras AnnaBerniceNo ratings yet
- BurnDocument25 pagesBurnNipul MondolNo ratings yet
- General ConsiderationsDocument14 pagesGeneral ConsiderationsAudree BustamanteNo ratings yet
- Burn PPT ShashiDocument4 pagesBurn PPT ShashiSachin KonkaniNo ratings yet
- Nursing - Burn InjuryDocument39 pagesNursing - Burn Injuryamaracha2003No ratings yet
- Burn CareDocument6 pagesBurn CareLeigh Chanelle OngNo ratings yet
- Perioperative Nursing: Prepared By: Annabeth K. Salonga RN, MANDocument67 pagesPerioperative Nursing: Prepared By: Annabeth K. Salonga RN, MANAnnabeth Kwong Salonga100% (2)
- Luka Bakar 2Document30 pagesLuka Bakar 2Yunita PanjaitanNo ratings yet
- Burn Injury: General Surgery Department, FKUI/RSCM, Jakarta, Indonesia, May 2011Document8 pagesBurn Injury: General Surgery Department, FKUI/RSCM, Jakarta, Indonesia, May 2011DeVi K. NinGsihNo ratings yet
- SURGERY For Nurses PDFDocument98 pagesSURGERY For Nurses PDFirene8000100% (1)
- 1 DR - Saif Principles of Infection 2021Document7 pages1 DR - Saif Principles of Infection 2021RihamNo ratings yet
- General Surgery: Post-Operative Care and ManagementDocument9 pagesGeneral Surgery: Post-Operative Care and ManagementMohammed Yousif AbdualjabbarNo ratings yet
- What Is Inflammation?: Cellular Response To InjuryDocument10 pagesWhat Is Inflammation?: Cellular Response To InjuryLalaine NadulpitNo ratings yet
- Burn NotesDocument5 pagesBurn NotespaulineorrNo ratings yet
- 4 Emergency and Mass Casualty NursingDocument7 pages4 Emergency and Mass Casualty NursingPxPPxH ChanNo ratings yet
- Operating Room ConceptsDocument47 pagesOperating Room ConceptsLoungayvan Batuyog100% (1)
- BurnsDocument31 pagesBurnsMUKESH SUNDARARAJAN100% (1)
- PeriopDocument48 pagesPeriopCherry Ann Garcia Durante100% (1)
- 4 Plenary: by Group 15CDocument42 pages4 Plenary: by Group 15CAulia RahmiNo ratings yet
- Burns: by S3 Unit Dept of Gen - Surgery AMCDocument31 pagesBurns: by S3 Unit Dept of Gen - Surgery AMCHyny P'gallaNo ratings yet
- CU. 9 BurnsDocument50 pagesCU. 9 BurnsCechanNo ratings yet
- Nursing Management of Patient With BurnsDocument30 pagesNursing Management of Patient With BurnsjsoalNo ratings yet
- Prone StudyDocument13 pagesProne StudySanketNandaniNo ratings yet
- Terjemahan KulitDocument5 pagesTerjemahan KulitErlieza Rosdania SupraptoNo ratings yet
- Emergency Medicine - Med RevisionsDocument69 pagesEmergency Medicine - Med RevisionsswamysamsonNo ratings yet
- 7-Postoperative Care and ComplicationsDocument25 pages7-Postoperative Care and ComplicationsAiden JosephatNo ratings yet
- BurnsDocument106 pagesBurnsShahini PrajapatiNo ratings yet
- Acute Biologic Crisis - Hand OutDocument48 pagesAcute Biologic Crisis - Hand OutLouis Carlos RoderosNo ratings yet
- Dr. Mirza Koeshardiandi ABC of BurnDocument35 pagesDr. Mirza Koeshardiandi ABC of Burnagus susantoNo ratings yet
- Perioperative Nursing: Mrs. Hilda V. Cruz, R.N.M.A.N (Instructor)Document135 pagesPerioperative Nursing: Mrs. Hilda V. Cruz, R.N.M.A.N (Instructor)Allen ElguiraNo ratings yet
- Burns Secret TestDocument2 pagesBurns Secret TestJessica KaelinNo ratings yet
- 1 2 2012med Surg BurnsDocument2 pages1 2 2012med Surg BurnsIan RamaNo ratings yet
- 9 - Post-OP Management and ComplicationsDocument57 pages9 - Post-OP Management and ComplicationsThon JustineNo ratings yet
- Appliedmicro Micro D& R AgamDocument83 pagesAppliedmicro Micro D& R Agamjanijkson29No ratings yet
- The Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNDocument52 pagesThe Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNrahmaya100% (1)
- Dr. Bivek Pokhrel Resident Medical Officer Annapurna Neurological Institute and Allied SciencesDocument21 pagesDr. Bivek Pokhrel Resident Medical Officer Annapurna Neurological Institute and Allied SciencesBivek PokhrelNo ratings yet
- Management of Patients With Burn Injury: Faculty: Rubina Shehzadi Nursing LecturerDocument42 pagesManagement of Patients With Burn Injury: Faculty: Rubina Shehzadi Nursing LecturerYou TuberNo ratings yet
- Focus Review For ATIDocument16 pagesFocus Review For ATIphandrew0892% (50)
- NEW Post Extubation Code JUN HUNGDocument18 pagesNEW Post Extubation Code JUN HUNGJun HungNo ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Clinical case in the emergency room of a patient with an ischemic strokeFrom EverandClinical case in the emergency room of a patient with an ischemic strokeNo ratings yet
- Hernia 2018Document5 pagesHernia 2018Razor GGNo ratings yet
- Curriculum Vitae: Name Date of Birth Nationality GMC NumberDocument13 pagesCurriculum Vitae: Name Date of Birth Nationality GMC NumberRazor GGNo ratings yet
- EliteArk Shop - Ark Shop ListDocument17 pagesEliteArk Shop - Ark Shop ListRazor GGNo ratings yet
- Social and Preventive MedicineDocument94 pagesSocial and Preventive MedicineRazor GGNo ratings yet
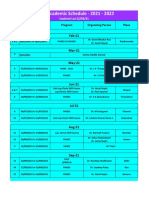
- IAGES Academic Schedule 2021Document2 pagesIAGES Academic Schedule 2021Razor GGNo ratings yet
- Fluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju AshokanDocument31 pagesFluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju Ashokanvaishnavi kaleNo ratings yet
- BurnsDocument80 pagesBurnsAlina IlovanNo ratings yet
- Fluid and Electrolytes, Balance and DisturbancesDocument157 pagesFluid and Electrolytes, Balance and DisturbancesDani PhilipNo ratings yet
- Module 8 SepsisDocument44 pagesModule 8 SepsisEstefania Cuta HernandezNo ratings yet
- ACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsDocument14 pagesACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsMara Medina - BorleoNo ratings yet
- AnzbaDocument1 pageAnzbaJeane SuyantoNo ratings yet
- Paper 3 Surgery Not Answered Till 2022Document288 pagesPaper 3 Surgery Not Answered Till 2022NEMO2322No ratings yet
- A Healthy Diet For A Badminton Player During Training & Competition - Joel Gayle School of BadmintonDocument3 pagesA Healthy Diet For A Badminton Player During Training & Competition - Joel Gayle School of BadmintonSumesh100% (1)
- Rectal FluidtherapyDocument7 pagesRectal FluidtherapyIan SabogalNo ratings yet
- Cme Fluid and Electrolytes 2902016Document37 pagesCme Fluid and Electrolytes 2902016Mohd Faie Ramli0% (1)
- Colloid PDFDocument45 pagesColloid PDFubaidrahamanNo ratings yet
- I.V. Fluid Therapy IDocument4 pagesI.V. Fluid Therapy IPrabath ChinthakaNo ratings yet
- Colloidal Solutions: Department of Medical Chemistry Pomeranian Medical UniversityDocument34 pagesColloidal Solutions: Department of Medical Chemistry Pomeranian Medical UniversityZaki PinjariNo ratings yet
- Prof. Mark Jheran Alvarez, USRN, MAN-MSDocument52 pagesProf. Mark Jheran Alvarez, USRN, MAN-MSMark Jheran AlvarezNo ratings yet
- ST Marks SolutionDocument2 pagesST Marks SolutionWawa HeeNo ratings yet
- 2040fe Part2Document15 pages2040fe Part2clubsingr28No ratings yet
- Approach To Severe Acute MalnutritionDocument49 pagesApproach To Severe Acute MalnutritionAlbertina Aipinge NandjilaNo ratings yet
- Restriction of Intravenous Fluids NejmDocument12 pagesRestriction of Intravenous Fluids NejmFrancisco Javier Gayoso DhagaNo ratings yet
- Gastro Inter It IsDocument3 pagesGastro Inter It IsDhea Imas WijayantiNo ratings yet
- CH 14 Test BankDocument21 pagesCH 14 Test BankKrestine Molle100% (1)
- Anestesia de Animales ExoticosDocument13 pagesAnestesia de Animales ExoticosDIANA MABEL PAGUAY CAJASNo ratings yet
- SWBCN011-Guideline - Initial Assessment and Management Burn Injury v2Document8 pagesSWBCN011-Guideline - Initial Assessment and Management Burn Injury v2Thanujaa UvarajNo ratings yet
- IV FluidDocument28 pagesIV FluidZulfkar Latief QadrieNo ratings yet
- Surgery and Perioperative Care: AnaestheticsDocument146 pagesSurgery and Perioperative Care: Anaestheticsjames.a.blairNo ratings yet
- Fluid Management: Basic ScienceDocument6 pagesFluid Management: Basic ScienceDjeddah Illarik NoriegaNo ratings yet
- Pancreatitis Guia JaponesaDocument6 pagesPancreatitis Guia JaponesaRonnyMercadoNo ratings yet