You might also like
- ICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomDocument3 pagesICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomvicndubNo ratings yet
- Esophageal DisordersDocument10 pagesEsophageal DisordersSheema ShNo ratings yet
- Definition and Etiology: PancreatitisDocument24 pagesDefinition and Etiology: PancreatitisAliyah Tofani PawelloiNo ratings yet
- Pre-Res Case Presentation: Jo Anne N. Ramos, MDDocument72 pagesPre-Res Case Presentation: Jo Anne N. Ramos, MDKah Mote KyuNo ratings yet
- Case Presentation: East Avenue Medical Center Female Surgical Ward Group DDocument32 pagesCase Presentation: East Avenue Medical Center Female Surgical Ward Group DKyle TampoyaNo ratings yet
- Responsesm To Metabolic Gi and Liver AlterationsDocument62 pagesResponsesm To Metabolic Gi and Liver AlterationsEdelen GaleNo ratings yet
- Gerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTDocument31 pagesGerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTRocky Willis100% (1)
- Short Written Mock 2021 Mn1 - AnsweredDocument20 pagesShort Written Mock 2021 Mn1 - AnsweredMatthew NgNo ratings yet
- VomitingDocument59 pagesVomitingزياد سعيدNo ratings yet
- Written Report 3Document4 pagesWritten Report 3Gabriel MillaNo ratings yet
- Medical Causes of Dysphagia - Evaluation and Diagnosis of GERD and Esophageal CancerDocument72 pagesMedical Causes of Dysphagia - Evaluation and Diagnosis of GERD and Esophageal CancerMaisarah IsmailNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Disorders of The StomachDocument26 pagesDisorders of The StomachAnnie Rose Dorothy MamingNo ratings yet
- Vague Complaint, Do Pregnancy Test, If Wretching Send To ER, If Chronic N/V Gi Issue Send To Get EvaluatedDocument5 pagesVague Complaint, Do Pregnancy Test, If Wretching Send To ER, If Chronic N/V Gi Issue Send To Get EvaluatedsadbgNo ratings yet
- Upper GI Guided NotesDocument9 pagesUpper GI Guided NotesVanessaNo ratings yet
- STUDY GUIDE N304 EXAM 1 My NotesDocument6 pagesSTUDY GUIDE N304 EXAM 1 My Notessoumya vadlamaniNo ratings yet
- Cholecystitis Case Study: Pathophysiology, Clinical Assessments, Nursing CareDocument61 pagesCholecystitis Case Study: Pathophysiology, Clinical Assessments, Nursing CarePlain GerlNo ratings yet
- d2 - Milla Telemed - Written Report 3Document4 pagesd2 - Milla Telemed - Written Report 3Gabriel MillaNo ratings yet
- CholelitiasisDocument42 pagesCholelitiasisEdwin YosuaNo ratings yet
- Common General Practice Consultations Notes For OSCEsDocument52 pagesCommon General Practice Consultations Notes For OSCEsNadia SalwaniNo ratings yet
- Pancreatitis Definition of TermsDocument6 pagesPancreatitis Definition of TermsDonna Marie Arguelles AmpaNo ratings yet
- Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Document62 pagesGatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Ardi PratamaNo ratings yet
- Common General Practice Consultations - Notes For OSCEsDocument53 pagesCommon General Practice Consultations - Notes For OSCEsChanel ClarkNo ratings yet
- Abdominal PainDocument26 pagesAbdominal Painsammy_d6No ratings yet
- GastrointestinalDocument63 pagesGastrointestinaljeshema100% (2)
- B6 - Surgery GS II Case 1Document9 pagesB6 - Surgery GS II Case 1GregNo ratings yet
- Case Presentation (IM)Document31 pagesCase Presentation (IM)WitneyGraceNo ratings yet
- It 2 - Signs and Symptoms of Git DisordersDocument54 pagesIt 2 - Signs and Symptoms of Git Disorderspikaanisa100% (9)
- Necrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualDocument3 pagesNecrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualJovvitaNo ratings yet
- Exam 1 Study GuideDocument3 pagesExam 1 Study GuideNataraj LoganathanNo ratings yet
- A Child With Prolonged FeverDocument38 pagesA Child With Prolonged FeverAly MorsyNo ratings yet
- Gastro NephroDocument93 pagesGastro Nephrohasanatiya41No ratings yet
- Power Git EndoDocument170 pagesPower Git Endoapi-3735995100% (1)
- GI System Physical Exam GuideDocument7 pagesGI System Physical Exam GuideS StPierreNo ratings yet
- Liver Nursing NotesDocument7 pagesLiver Nursing NotesHeather ShantaeNo ratings yet
- Assessment of Metabolic and Gastrointestinal, Liver AlterationsDocument10 pagesAssessment of Metabolic and Gastrointestinal, Liver AlterationsGel JamsNo ratings yet
- Case PresentationDocument22 pagesCase PresentationVikaNo ratings yet
- GI, GU, Hepatobiliary, Endo HandoutsDocument18 pagesGI, GU, Hepatobiliary, Endo HandoutsCharlie MoquiteNo ratings yet
- GROUP 3 Case PresentationDocument35 pagesGROUP 3 Case PresentationDinesh KumarNo ratings yet
- Alimentary and Biliary Conditions 3-1Document249 pagesAlimentary and Biliary Conditions 3-1Mercy KeruboNo ratings yet
- VomitingDocument4 pagesVomitingMax BrownNo ratings yet
- Abdominal PainDocument6 pagesAbdominal PainMatthieu FortinNo ratings yet
- PancreatitisDocument3 pagesPancreatitisSalma NazarNo ratings yet
- Abdominal Case Study CompiledDocument392 pagesAbdominal Case Study CompiledIshak IzharNo ratings yet
- Nursing MGT of PT With Lower Git DisordersDocument65 pagesNursing MGT of PT With Lower Git DisordersCarlos LorenzoNo ratings yet
- Nausea VomitingDocument36 pagesNausea VomitingDian Fitri100% (1)
- M1 MET1 SG ACaseofAcuteCholecystitisDocument14 pagesM1 MET1 SG ACaseofAcuteCholecystitisNicholas ReljaNo ratings yet
- Acute and Chronic DiarrhoeaDocument20 pagesAcute and Chronic DiarrhoeaVipul Nagnesia100% (2)
- PPT 4 CARE OF CLIENTS WITH IBS MALABSORP ULCERATIVE COLITIS CROHNS FINAL COPYDocument35 pagesPPT 4 CARE OF CLIENTS WITH IBS MALABSORP ULCERATIVE COLITIS CROHNS FINAL COPYevren yilmazNo ratings yet
- Nursing Patho CardsDocument195 pagesNursing Patho Cardsgiogmail100% (1)
- Acute Abdominal PainDocument5 pagesAcute Abdominal PainLM Mys100% (1)
- Gastroduodenal Disorders: Suazo, Trisha Mae S. 3BSN-ADocument12 pagesGastroduodenal Disorders: Suazo, Trisha Mae S. 3BSN-AKenneth OpinaNo ratings yet
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- NCMB 316 Cu11 Liver, Pancreas, & GallbladderDocument74 pagesNCMB 316 Cu11 Liver, Pancreas, & GallbladderJanine Dela CruzNo ratings yet
- RSVDocument15 pagesRSVbtheresakNo ratings yet
- Acute & Chronic Pancreatitis GuideDocument38 pagesAcute & Chronic Pancreatitis GuideAliyah Tofani PawelloiNo ratings yet
- DyspepsiaDocument18 pagesDyspepsiaMaya DibrinaNo ratings yet
- Lower GI Chapter Summary: Constipation, Diarrhea, Appendicitis & MoreDocument8 pagesLower GI Chapter Summary: Constipation, Diarrhea, Appendicitis & MoreRebeccaNo ratings yet
- Simman: Where Are You? What Are You Expecting To Find There?Document6 pagesSimman: Where Are You? What Are You Expecting To Find There?muradkhanNo ratings yet
- Breaking Bad NewsDocument15 pagesBreaking Bad NewsmuradkhanNo ratings yet
- Back PainDocument13 pagesBack PainmuradkhanNo ratings yet
- Chest PainDocument14 pagesChest PainmuradkhanNo ratings yet
- Ear, Nose and Throat: Dr. Mo SobhyDocument34 pagesEar, Nose and Throat: Dr. Mo SobhymuradkhanNo ratings yet
- The Pan StationsDocument14 pagesThe Pan StationsmuradkhanNo ratings yet
- Manage tiredness and sleep apnea with lifestyle changes and CPAP therapyDocument23 pagesManage tiredness and sleep apnea with lifestyle changes and CPAP therapymuradkhanNo ratings yet
- ThyroidDocument17 pagesThyroidmuradkhanNo ratings yet
- DR Mo Q BankDocument137 pagesDR Mo Q BankmuradkhanNo ratings yet
- TransgenderDocument10 pagesTransgendermuradkhanNo ratings yet
- GeM Bidding 3702669Document10 pagesGeM Bidding 3702669ANIMESH JAINNo ratings yet
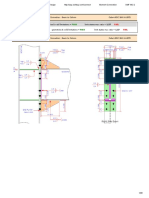
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)
- Course Code Part Sem Paper Code Paper NameDocument3 pagesCourse Code Part Sem Paper Code Paper Nameshiv mishraNo ratings yet
- Economics Principles and Policy 13th Edition Baumol Solutions ManualDocument2 pagesEconomics Principles and Policy 13th Edition Baumol Solutions ManualCraigGonzalezaxzgd100% (17)
- Ffective Riting Kills: Training & Discussion OnDocument37 pagesFfective Riting Kills: Training & Discussion OnKasi ReddyNo ratings yet
- ErgonomicsDocument15 pagesErgonomicsdtmNo ratings yet
- MPMC All Questions and AnswerDocument6 pagesMPMC All Questions and AnswerMODERN TELUGAMMAYINo ratings yet
- Islamic Center Design With Islamic ArchiDocument11 pagesIslamic Center Design With Islamic ArchiMuhammad Sufiyan SharafudeenNo ratings yet
- ECOSYS M2030dn M2530dn M2035dn M2535dn SM UKDocument273 pagesECOSYS M2030dn M2530dn M2035dn M2535dn SM UKMaks Prost60% (5)
- Examining The Structural Relationships of Destination Image, Tourist Satisfaction PDFDocument13 pagesExamining The Structural Relationships of Destination Image, Tourist Satisfaction PDFAndreea JecuNo ratings yet
- PTR01 21050 90inst PDFDocument40 pagesPTR01 21050 90inst PDFЯн ПавловецNo ratings yet
- Sony STR Da80esDocument66 pagesSony STR Da80estelstarservicesNo ratings yet
- Coaching, Mentoring & OnboardingDocument43 pagesCoaching, Mentoring & OnboardingosvehNo ratings yet
- Nursing Care Plans for ChildrenDocument4 pagesNursing Care Plans for ChildrenAlexander Rodriguez OlipasNo ratings yet
- GCS Activity 2003Document33 pagesGCS Activity 2003donnottryNo ratings yet
- COVID-19 and Flu Vaccination Walgreens Immunization ServicesDocument1 pageCOVID-19 and Flu Vaccination Walgreens Immunization ServicesAitana MaldonadoNo ratings yet
- Conditions For The Emergence of Life On The Early Earth: Summary and ReflectionsDocument15 pagesConditions For The Emergence of Life On The Early Earth: Summary and Reflectionsapi-3713202No ratings yet
- The Separation of Coherent and Incoherent Compton X-Ray ScatteringDocument8 pagesThe Separation of Coherent and Incoherent Compton X-Ray ScatteringFaisal AmirNo ratings yet
- Overview of Research ProcessDocument31 pagesOverview of Research Processprema balusamyNo ratings yet
- wizBRAINeng20 2Document4 pageswizBRAINeng20 2Deepika AgrawalNo ratings yet
- Engineering Design For A Circular Economy - A List of Design GuidelinesDocument1 pageEngineering Design For A Circular Economy - A List of Design Guidelinesmy oneNo ratings yet
- A Rite of SpringDocument10 pagesA Rite of SpringLucius Gregory MeredithNo ratings yet
- Chapter 22A - Sound WavesDocument24 pagesChapter 22A - Sound Wavesqwivy.comNo ratings yet
- Bee WareDocument49 pagesBee WareJayNo ratings yet
- Sapamine CSN Textile Softener: Technical Data SheetDocument5 pagesSapamine CSN Textile Softener: Technical Data SheetsaskoNo ratings yet
- Research 10 Mod2Document28 pagesResearch 10 Mod2Fernadez RodisonNo ratings yet
- 5.test Report - RFU-C-7Ghz IP10 Extract VersionDocument42 pages5.test Report - RFU-C-7Ghz IP10 Extract Versionminhdung.pham4713No ratings yet
- Nord Stage Factory Patches v3 v4 v5Document18 pagesNord Stage Factory Patches v3 v4 v5Danilo Giuliani DobermannNo ratings yet
- Quality Control and Quality AssuranceDocument7 pagesQuality Control and Quality AssuranceMoeen Khan Risaldar100% (1)
- Filipino Nationalism LessonDocument24 pagesFilipino Nationalism LessonIan Jay TumulakNo ratings yet