You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- AAN 204 CARDIOVASCULAR NURSING COURSEWORKDocument118 pagesAAN 204 CARDIOVASCULAR NURSING COURSEWORKLucian CaelumNo ratings yet
- Dysrhythmia InterpretationDocument56 pagesDysrhythmia InterpretationgerajassoNo ratings yet
- Coronary Artery Disease & Hypertension Practice Quiz (50 Questions)Document18 pagesCoronary Artery Disease & Hypertension Practice Quiz (50 Questions)Erica Veluz LuyunNo ratings yet
- Central Venous Pressure MonitoringDocument13 pagesCentral Venous Pressure MonitoringKris TejereroNo ratings yet
- Inotropes and Vasoconstictor PackageDocument25 pagesInotropes and Vasoconstictor PackageYoussef MokdadNo ratings yet
- Cardiac Output, Venous Return, and Their RegulationDocument50 pagesCardiac Output, Venous Return, and Their RegulationMohammed T. Abdul Razak100% (1)
- Heart Lung InteractionDocument29 pagesHeart Lung InteractionKARDIOLOGI STASE RSALNo ratings yet
- Mecanical VentilationDocument433 pagesMecanical Ventilationmihaela popescuNo ratings yet
- Hemodynamic Monitoring EssentialsDocument35 pagesHemodynamic Monitoring EssentialsWiz SamNo ratings yet
- Evidence For Varicose Vein Treatment An Overview ofDocument9 pagesEvidence For Varicose Vein Treatment An Overview oflucyishakNo ratings yet
- Tergeted Temperature #Document10 pagesTergeted Temperature #lucyishakNo ratings yet
- Daftar Harga BarangDocument1 pageDaftar Harga BaranglucyishakNo ratings yet
- Daftar Calon Santri Muallimin Yang Dinyatakan LulusDocument2 pagesDaftar Calon Santri Muallimin Yang Dinyatakan LuluslucyishakNo ratings yet
- Jr. CARDIAC ARREST (CA)Document28 pagesJr. CARDIAC ARREST (CA)lucyishakNo ratings yet
- Current Management of Varicose Veins ReviewDocument4 pagesCurrent Management of Varicose Veins ReviewlucyishakNo ratings yet
- Endovascular Management of Varicose VeinsDocument7 pagesEndovascular Management of Varicose VeinslucyishakNo ratings yet
- Timing VSRDocument8 pagesTiming VSRlucyishakNo ratings yet
- Clinical Presentation of Varicose VeinsDocument8 pagesClinical Presentation of Varicose VeinslucyishakNo ratings yet
- Intravenous Iron Therapy and The Cardiovascular System - KARDIODocument10 pagesIntravenous Iron Therapy and The Cardiovascular System - KARDIOlucyishakNo ratings yet
- Epidemiological, Life Style, and Occupational Factors Associated With Lower Limb Varicose VeinsDocument11 pagesEpidemiological, Life Style, and Occupational Factors Associated With Lower Limb Varicose VeinslucyishakNo ratings yet
- 1994 Diagnosis and Treatment of Varicose Veins A ReviewDocument21 pages1994 Diagnosis and Treatment of Varicose Veins A ReviewlucyishakNo ratings yet
- Cardiovascular Disease PreventionDocument111 pagesCardiovascular Disease PreventionlucyishakNo ratings yet
- Jurnal Diadnostik Dan Management Pancreatic CancerDocument8 pagesJurnal Diadnostik Dan Management Pancreatic CancerlucyishakNo ratings yet
- Jurnal Tumor Metastasis Paru Hepar Dari PancreasDocument15 pagesJurnal Tumor Metastasis Paru Hepar Dari PancreaslucyishakNo ratings yet
- Jurnal 1 LusyDocument9 pagesJurnal 1 LusylucyishakNo ratings yet
- Pembagian Jadwal Stase GHDocument2 pagesPembagian Jadwal Stase GHlucyishakNo ratings yet
- Tatalaksana Aortic RegurgitationDocument3 pagesTatalaksana Aortic RegurgitationlucyishakNo ratings yet
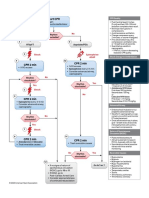
- Adult Cardiac Arrest Algorithm: VF/PVT Asystole/PEADocument1 pageAdult Cardiac Arrest Algorithm: VF/PVT Asystole/PEARamos SiahaanNo ratings yet
- Tugas PAKAR - Pemeriksaan Fisis Aorta StenosisDocument10 pagesTugas PAKAR - Pemeriksaan Fisis Aorta StenosislucyishakNo ratings yet
- Link SCUDocument2 pagesLink SCUlucyishakNo ratings yet
- Link SCUDocument2 pagesLink SCUlucyishakNo ratings yet
- Stroke Volume and Cardiac OutputDocument9 pagesStroke Volume and Cardiac OutputAyi Abdul BasithNo ratings yet
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- Ccu First Quiz FinalDocument4 pagesCcu First Quiz FinalEggy PascualNo ratings yet
- Types of ShocksDocument33 pagesTypes of Shocksmark OrpillaNo ratings yet
- 8c99f2 PDFDocument52 pages8c99f2 PDFKrisParadajsNo ratings yet
- Right Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Document9 pagesRight Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Trần Quang HuyNo ratings yet
- OutputDocument12 pagesOutputzenishzalamNo ratings yet
- Chapter 5 Cardiac Output and The Pressure-Volume RelationshipDocument15 pagesChapter 5 Cardiac Output and The Pressure-Volume Relationshipaisyahasrii_No ratings yet
- Update - in AnestesiaDocument200 pagesUpdate - in AnestesiaInês MendonçaNo ratings yet
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- My Lecture13 - Cardiovascular PhysiologyDocument16 pagesMy Lecture13 - Cardiovascular PhysiologyVivek ChaudharyNo ratings yet
- Cardiac Out PutDocument18 pagesCardiac Out PutShaells JoshiNo ratings yet
- Heart Lung InteractionDocument39 pagesHeart Lung InteractionziadNo ratings yet
- Dilated Cardiomyopathy Notes AtfDocument15 pagesDilated Cardiomyopathy Notes AtfSingha ChangsiriwatanaNo ratings yet
- Cardiac Output: Ejection Fraction (EF%)Document5 pagesCardiac Output: Ejection Fraction (EF%)JockerNo ratings yet
- Congestive Heart FailureDocument43 pagesCongestive Heart Failure568563100% (1)
- Dynamic Hemodynamic Monitoring Assesses Cardiovascular SufficiencyDocument23 pagesDynamic Hemodynamic Monitoring Assesses Cardiovascular SufficiencyJuan CarrascoNo ratings yet
- Cardiogenic Shock NclexDocument81 pagesCardiogenic Shock NclexKrishna SapkotaNo ratings yet
- Principles of Invasive HemodynamicsDocument18 pagesPrinciples of Invasive HemodynamicsShreya SinhaNo ratings yet
- Will This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Document12 pagesWill This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Roberto López MataNo ratings yet
- Owner's Manual: Öhlins Cartridge Kit For MX & EnduroDocument12 pagesOwner's Manual: Öhlins Cartridge Kit For MX & EnduroНикола КарагьозовNo ratings yet