You might also like
- Upper Gastrointestinal Bleeding in Children in Southern IranDocument4 pagesUpper Gastrointestinal Bleeding in Children in Southern Iranzuryati mdiNo ratings yet
- 134 FullDocument12 pages134 FullJuwita PratiwiNo ratings yet
- Approach To A Child With Upper Gastrointestinal BleedingDocument8 pagesApproach To A Child With Upper Gastrointestinal Bleedingzuryati mdiNo ratings yet
- The Causes of Upper Gastrointestinal Bleeding in The National Referral Hospital: Evaluation On Upper Gastrointestinal Tract Endoscopic Result in Five Years PeriodDocument4 pagesThe Causes of Upper Gastrointestinal Bleeding in The National Referral Hospital: Evaluation On Upper Gastrointestinal Tract Endoscopic Result in Five Years PeriodSyawal PratamaNo ratings yet
- Ugib 1Document12 pagesUgib 1Mutiara FauzaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- 404 398 1 SMDocument4 pages404 398 1 SMfak youNo ratings yet
- Research Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaDocument7 pagesResearch Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaKurnia pralisaNo ratings yet
- Bloody Stool Journal 2Document8 pagesBloody Stool Journal 2dr.herusetiawanNo ratings yet
- Ascites in Patients With Noncirrhotic Nonmalignant Extrahepatic Portal Vein ThrombosisDocument6 pagesAscites in Patients With Noncirrhotic Nonmalignant Extrahepatic Portal Vein ThrombosisAngeliuz TimoteoNo ratings yet
- Diagnosis and Management of Upper Gastrointestinal Bleeding in ChildrenDocument12 pagesDiagnosis and Management of Upper Gastrointestinal Bleeding in ChildrenYoga ForeverrNo ratings yet
- Electronic Physician (ISSN: 2008-5842)Document5 pagesElectronic Physician (ISSN: 2008-5842)Aldian DianNo ratings yet
- 11 134 v12n4 2013 PredictingPortalDocument11 pages11 134 v12n4 2013 PredictingPortalDevy Widiya GrafitasariNo ratings yet
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- CMQ 008Document3 pagesCMQ 008itsshaswatNo ratings yet
- Ileus and Intestinal Obstruction - Comparison Between Children and AdultsDocument5 pagesIleus and Intestinal Obstruction - Comparison Between Children and Adultsaliy_drNo ratings yet
- Paediatric Appendicitis Scoring: A Useful Guide To Diagnose Acute Appendicitis in ChildrenDocument6 pagesPaediatric Appendicitis Scoring: A Useful Guide To Diagnose Acute Appendicitis in ChildrenFebrian Naranggi Aradia PutraNo ratings yet
- SudaniwawiDocument7 pagesSudaniwawiMouhammed SleiayNo ratings yet
- Etiological Pattern and Outcome of Non-Variceal Upper G.I. BleedingDocument5 pagesEtiological Pattern and Outcome of Non-Variceal Upper G.I. BleedingJawad ZafarNo ratings yet
- Post Cholecystectomy Syndrome in Pediatric PatientDocument4 pagesPost Cholecystectomy Syndrome in Pediatric PatientzerojcNo ratings yet
- Acalculous Cholecystitis Prevalence On Abdominal Ultrasonography Examination of HIV/HCV Co-Infection Patients in Cipto Mangunkusumo HospitalDocument3 pagesAcalculous Cholecystitis Prevalence On Abdominal Ultrasonography Examination of HIV/HCV Co-Infection Patients in Cipto Mangunkusumo HospitalDiga AlbrianNo ratings yet
- Peptic UlcerDocument3 pagesPeptic UlcerzikraalfaNo ratings yet
- Ehbo PDFDocument8 pagesEhbo PDFEngidaNo ratings yet
- Article ReviewDocument8 pagesArticle Reviewwjohnson_3No ratings yet
- Clinical Profile of Patients With Obstructive Jaundice: A Surgeon's PerspectivesDocument5 pagesClinical Profile of Patients With Obstructive Jaundice: A Surgeon's Perspectivessitoxpadang ceriaNo ratings yet
- 403 396 1 SMDocument8 pages403 396 1 SMichaNo ratings yet
- Journal of Pediatric Surgery: Wendy K. Fujioka, Robert A. CowlesDocument3 pagesJournal of Pediatric Surgery: Wendy K. Fujioka, Robert A. CowlesVmiguel LcastilloNo ratings yet
- Development of Type I Gastric Carcinoid in Patients With Chronic Atrophic GastritisDocument9 pagesDevelopment of Type I Gastric Carcinoid in Patients With Chronic Atrophic GastritisAbristaSeptikasariNo ratings yet
- Colitis: A Practical Approach to Colon and Ileum Biopsy InterpretationFrom EverandColitis: A Practical Approach to Colon and Ileum Biopsy InterpretationAnne Jouret-MourinNo ratings yet
- Validity of Upper Gastrointestinal Bleeding Etiology Score For Determining Variceal Bleeding by Doing Esophagoduodenoscopy As Gold StandardDocument4 pagesValidity of Upper Gastrointestinal Bleeding Etiology Score For Determining Variceal Bleeding by Doing Esophagoduodenoscopy As Gold StandardsmallheartNo ratings yet
- Gastroschisis and Omphalocele PDFDocument8 pagesGastroschisis and Omphalocele PDFUtama puteraNo ratings yet
- Infantile Hypertrophic Pyloric Stenosis: A Single Institution's ExperienceDocument3 pagesInfantile Hypertrophic Pyloric Stenosis: A Single Institution's ExperienceTeuku FennyNo ratings yet
- Management of Liver Abscess in Children: Our Experience: 10.5005/jp-Journals-10018-1206Document4 pagesManagement of Liver Abscess in Children: Our Experience: 10.5005/jp-Journals-10018-1206Ivan VeriswanNo ratings yet
- Poddar 2018Document6 pagesPoddar 2018AfniNo ratings yet
- Urinary and Fecal Continence in Adolescent and Adult Patients With Cloacal Exstrophy 2022Document7 pagesUrinary and Fecal Continence in Adolescent and Adult Patients With Cloacal Exstrophy 2022Oscar Sanchez ParisNo ratings yet
- JR DAZ Digestif Senior - Hirschsprung's Complication JurnalDocument8 pagesJR DAZ Digestif Senior - Hirschsprung's Complication Jurnaldiaz.azpNo ratings yet
- Pediatric Gastroesophageal Reflux DiseaseDocument5 pagesPediatric Gastroesophageal Reflux Diseasegemala wahabNo ratings yet
- Current Success in The Treatment of Intussusception in ChildrenDocument9 pagesCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniNo ratings yet
- 6665 PDFDocument4 pages6665 PDFerindah puspowatiNo ratings yet
- Clinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingDocument8 pagesClinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingLaura Anghel-MocanuNo ratings yet
- Laparotomy in Children in A Tertiary Hospital in A Developing CountryDocument5 pagesLaparotomy in Children in A Tertiary Hospital in A Developing CountryWorld Journal of Clinical SurgeryNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverBlackHAT GAMINGNo ratings yet
- Use of White Blood Cell Count and Negative Appendectomy RateDocument8 pagesUse of White Blood Cell Count and Negative Appendectomy RatePremaKurniaNo ratings yet
- 136929-Article Text-366218-1-10-20160603Document6 pages136929-Article Text-366218-1-10-20160603Sulabh ShresthaNo ratings yet
- Childhood Acute Pancreatitis in A Children's Hospital: S-K Goh, C H Chui, A S JacobsenDocument4 pagesChildhood Acute Pancreatitis in A Children's Hospital: S-K Goh, C H Chui, A S Jacobsentalenthero9xNo ratings yet
- Stevens JohsonDocument8 pagesStevens JohsonDaily RomeroNo ratings yet
- Prevalence of Hiatal Hernia and Achalasia - V0 11-06-20Document25 pagesPrevalence of Hiatal Hernia and Achalasia - V0 11-06-20AlfonsoSánchezNo ratings yet
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Per-Operative Conversion of Laparoscopic Cholecystectomy To Open Surgery: Prospective Study at JSS Teaching Hospital, Karnataka, IndiaDocument5 pagesPer-Operative Conversion of Laparoscopic Cholecystectomy To Open Surgery: Prospective Study at JSS Teaching Hospital, Karnataka, IndiaSupriya PonsinghNo ratings yet
- Evaluation and Management of Cholelithiasis in Children: A Hospital Based StudyDocument6 pagesEvaluation and Management of Cholelithiasis in Children: A Hospital Based StudyangelaanapakuNo ratings yet
- Belsha2016 - INdication of EndosDocument9 pagesBelsha2016 - INdication of EndosThinh NguyenNo ratings yet
- Prevalensi Dan Faktor AsosiasiDocument11 pagesPrevalensi Dan Faktor Asosiasisahama2508No ratings yet
- Gastrointestinal Bleeding The Pediatric Patient: BrightDocument13 pagesGastrointestinal Bleeding The Pediatric Patient: BrightTimothy Eduard A. SupitNo ratings yet
- Prevalence of Variceal Bleeding in ALD PatientsDocument5 pagesPrevalence of Variceal Bleeding in ALD PatientsvarishNo ratings yet
- Eng 2014Document6 pagesEng 2014Ahmad NurdiansyahNo ratings yet
- Toddler's Diarrhea: Is It An Under-Recognized Entity in Developing Countries?Document6 pagesToddler's Diarrhea: Is It An Under-Recognized Entity in Developing Countries?deonardNo ratings yet
- Wireless Capsule Video EndosDocument3 pagesWireless Capsule Video EndoslayasureNo ratings yet
- Indeks Diastase 2 PDFDocument5 pagesIndeks Diastase 2 PDFddew indahNo ratings yet
- Endoscopic Hemostasis in Intensive Care Unit Patients With Upper Digestive Tract BleedingDocument7 pagesEndoscopic Hemostasis in Intensive Care Unit Patients With Upper Digestive Tract BleedingAgung KaryawinaraNo ratings yet
- Types Sites and Causes of Mechanical Intestinal ObDocument5 pagesTypes Sites and Causes of Mechanical Intestinal ObPutra FebdianNo ratings yet
- Pediatric Gastrointestinal Bleeding Perspectives FDocument12 pagesPediatric Gastrointestinal Bleeding Perspectives FAsfiani PediatricianNo ratings yet
- Management of Upper Gastro Intestinal BleedingDocument9 pagesManagement of Upper Gastro Intestinal BleedingAsfiani PediatricianNo ratings yet
- Acute Upper Gi Bleeding, Predict Need For Endoscopic TherapyDocument5 pagesAcute Upper Gi Bleeding, Predict Need For Endoscopic TherapyAsfiani PediatricianNo ratings yet
- Asianjpediatrnephrol1138 2513254 065852Document3 pagesAsianjpediatrnephrol1138 2513254 065852Asfiani PediatricianNo ratings yet
- F. M. Busby - The Breeds of Man PDFDocument317 pagesF. M. Busby - The Breeds of Man PDFlion clarenceNo ratings yet
- Birth TraumaDocument57 pagesBirth TraumaAbu HajerahNo ratings yet
- TB - SeminarDocument12 pagesTB - SeminarLaith DmourNo ratings yet
- Approach To The Patient With Postmenopausal Uterine Bleeding - UpToDateDocument18 pagesApproach To The Patient With Postmenopausal Uterine Bleeding - UpToDateCHINDY REPA REPANo ratings yet
- NENC Regional SGLT2 Top Tips v1.2 NTAG Approved March 2023Document5 pagesNENC Regional SGLT2 Top Tips v1.2 NTAG Approved March 2023Nehal ElnagarNo ratings yet
- 01 Staff Nurse AIIMS Rishikesh Memory Based QuestionDocument2 pages01 Staff Nurse AIIMS Rishikesh Memory Based QuestionDip Ayan MNo ratings yet
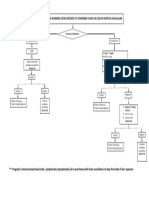
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- Typhoid WidalDocument4 pagesTyphoid WidalamaliamldNo ratings yet
- Sitz Bath Procedure ChecklistDocument4 pagesSitz Bath Procedure ChecklistGeno Adrian T Pampanga100% (1)
- TuberculosisDocument4 pagesTuberculosisMjel Kezhia BarrietaNo ratings yet
- Eapp Act.1Document2 pagesEapp Act.1cherish mae oconNo ratings yet
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Discharge Plan For TuberculosisDocument6 pagesDischarge Plan For Tuberculosisploy8No ratings yet
- ملخص عن حب الشبابDocument10 pagesملخص عن حب الشبابMohammadSAL-RawashdehNo ratings yet
- SP234 Bird GuanoDocument3 pagesSP234 Bird GuanoJohn GeddesNo ratings yet
- Shivna Thesis PerformaDocument13 pagesShivna Thesis Performasarjak shahNo ratings yet
- History of MedicineDocument108 pagesHistory of MedicineAlexandra Constantin100% (2)
- TURNER SYNDROME HandoutsDocument7 pagesTURNER SYNDROME HandoutsMaria Donabella OngueNo ratings yet
- Psy 119 Lec 1Document2 pagesPsy 119 Lec 1Angelo SumaoyNo ratings yet
- Hyperbilirubinemia ManagementDocument37 pagesHyperbilirubinemia ManagementkaerickaericNo ratings yet
- Abnormal Platelet Activity in Dogs and Cats - Impact and MeasurementDocument16 pagesAbnormal Platelet Activity in Dogs and Cats - Impact and MeasurementViviana Castillo VanegasNo ratings yet
- Sysmex SEED Haematology InflammatoryDocument7 pagesSysmex SEED Haematology InflammatoryTzeto Han CongNo ratings yet
- DRUG STUDY ClonazepamDocument2 pagesDRUG STUDY ClonazepamP BNo ratings yet
- Drug Profiling PHARMACOLOGYDocument71 pagesDrug Profiling PHARMACOLOGYJay MagsaysayNo ratings yet
- Anxiolytics and AntidepressantsDocument271 pagesAnxiolytics and AntidepressantsAmir PeljtoNo ratings yet
- Oxygen AdministrationDocument25 pagesOxygen Administrationkirutheka nithilaaNo ratings yet
- Thyrotoxic Periodic Paralysis A Case Study and Review of The LiteratureDocument5 pagesThyrotoxic Periodic Paralysis A Case Study and Review of The LiteratureEvin Komala DewiNo ratings yet
- Oscillopsia Is The Illusion of Oscillation of The Visual Surroundings While Vertigo Refers To A Sense of Spinning or Other Motion That May Be PhysiologicalDocument2 pagesOscillopsia Is The Illusion of Oscillation of The Visual Surroundings While Vertigo Refers To A Sense of Spinning or Other Motion That May Be PhysiologicalRubie Ann TillorNo ratings yet
- Drug StudyDocument4 pagesDrug Studym100% (1)
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYDocument5 pagesUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)