You might also like
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dysfunkcja Narzadu RuchuDocument140 pagesDysfunkcja Narzadu RuchuRobNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Curriculum Ampliado II - ContenidosDocument181 pagesCurriculum Ampliado II - Contenidospapeleria GoMartNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Writ Petition Steel FlyoverDocument28 pagesWrit Petition Steel FlyoverFirstpostNo ratings yet
- Formato de Reporte de Entrevista FamiliarDocument4 pagesFormato de Reporte de Entrevista FamiliarLiliann RiveraNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Nursing Exam For Review With RationaleDocument39 pagesNursing Exam For Review With RationaleKeizha Ronatay100% (2)
- Caderno de AtividadesDocument10 pagesCaderno de AtividadespratamariliaNo ratings yet
- DifteriaDocument28 pagesDifteriaErika Ortega Galindo100% (1)
- DOC-SST-003 Línea Base Del Sistema de Seguridad y Salud en El Trabajo v1Document21 pagesDOC-SST-003 Línea Base Del Sistema de Seguridad y Salud en El Trabajo v1Lening09No ratings yet
- Protocolo de Enfermeria en Trabajo de PartoDocument57 pagesProtocolo de Enfermeria en Trabajo de PartoLiz EspinozaNo ratings yet
- Advancing Palliative Care in The Public Sector - DrRichardLimDocument26 pagesAdvancing Palliative Care in The Public Sector - DrRichardLimmalaysianhospicecouncil6240100% (1)
- The Buddhist Art of ManifestationDocument65 pagesThe Buddhist Art of Manifestation28buck100% (1)
- 036 Sera Con P - AB - MSDS - E - 270916Document10 pages036 Sera Con P - AB - MSDS - E - 270916Anggit AdiyanaNo ratings yet
- Informe PsicologicoDocument7 pagesInforme PsicologicoRusooRodriguezNo ratings yet
- Atendimento Educacional - Doenças RarasDocument11 pagesAtendimento Educacional - Doenças RarasAna Cristina Marinho da SilvaNo ratings yet
- Higienismo SuperinteressanteDocument7 pagesHigienismo SuperinteressanteGustavo MantegaNo ratings yet
- Clasificacion de Los AlimentosDocument3 pagesClasificacion de Los AlimentosFriida Fernanda'No ratings yet
- Atypical Ductal HyperplasiaDocument6 pagesAtypical Ductal HyperplasiapgalamilloNo ratings yet
- Indicadores de SaludDocument3 pagesIndicadores de SaludLaleska Godoy0% (1)
- LagundiDocument3 pagesLagundiCarlaNo ratings yet
- Camp Report 123Document20 pagesCamp Report 123nabin xthNo ratings yet
- Parent/ Consent Form: Boy Scouts of The Philippines Sultan Kudarat Council Lutayan District II Boy'S Application FormDocument4 pagesParent/ Consent Form: Boy Scouts of The Philippines Sultan Kudarat Council Lutayan District II Boy'S Application FormEdward Jr. PorrasNo ratings yet
- 12 Hábitos para Una Vida SaludableDocument6 pages12 Hábitos para Una Vida SaludableSimpsonmania LatinoAmericaNo ratings yet
- PARECER Ao MPTDocument11 pagesPARECER Ao MPTFelipe NunesNo ratings yet
- Proceeding Icgh Aic-Hhc 2019 (Draft)Document291 pagesProceeding Icgh Aic-Hhc 2019 (Draft)deny gunawanNo ratings yet
- Taller No.1 Matriz de Riesgos y Oportunidades SSTDocument77 pagesTaller No.1 Matriz de Riesgos y Oportunidades SSTLeonardo HerreraNo ratings yet
- 4 Fisioartículo Esguince TobilloDocument5 pages4 Fisioartículo Esguince TobilloUriel BachurNo ratings yet
- Malla Curricular Propuesta Programacion Revisada 0.3 GF 1Document1 pageMalla Curricular Propuesta Programacion Revisada 0.3 GF 1ALICIA ELIZABETH DELEON ORTIZNo ratings yet
- Informe Linder TDocument5 pagesInforme Linder TLinder Tapia ChumbeNo ratings yet
- Alimentación Enteral Y ParenteralDocument4 pagesAlimentación Enteral Y ParenteralEsthelis SanabriaNo ratings yet
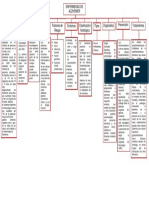
- TAREA #02 - ENFERMEDAD DEL ALZHEIMER (Elaborar Un Organizador Visual)Document1 pageTAREA #02 - ENFERMEDAD DEL ALZHEIMER (Elaborar Un Organizador Visual)ANGELA JULISA COPA EDUARDONo ratings yet