You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Daftar Manfaat Rawat Jalan Gol 3 3713102300032 1673238831Document1 pageDaftar Manfaat Rawat Jalan Gol 3 3713102300032 1673238831wahyunurrizkyNo ratings yet
- PT Way Tech Indonesia: QUOTATION No: 02.Q1722IP - BTRDocument1 pagePT Way Tech Indonesia: QUOTATION No: 02.Q1722IP - BTRwahyunurrizkyNo ratings yet
- Quotation VMI N°20113284 of 10.02.2020Document4 pagesQuotation VMI N°20113284 of 10.02.2020wahyunurrizkyNo ratings yet
- Laboratory English 0Document80 pagesLaboratory English 0wahyunurrizkyNo ratings yet
- A6erffierm: To The Authorities of INDONESIADocument1 pageA6erffierm: To The Authorities of INDONESIAwahyunurrizkyNo ratings yet
- Dokumen Training AK3 KimiaDocument3 pagesDokumen Training AK3 KimiawahyunurrizkyNo ratings yet
- Dokumen Training AK3 ListrikDocument4 pagesDokumen Training AK3 ListrikwahyunurrizkyNo ratings yet
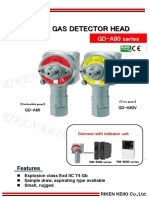
- Riken Gas Detector Head: GD-A80 SeriesDocument2 pagesRiken Gas Detector Head: GD-A80 SerieswahyunurrizkyNo ratings yet
- Enofa - 2022Document1 pageEnofa - 2022wahyunurrizkyNo ratings yet
- Terms and Conditions For The Sale of ProductsDocument4 pagesTerms and Conditions For The Sale of ProductswahyunurrizkyNo ratings yet
- NPWP - Indodaya Cipta LestariDocument1 pageNPWP - Indodaya Cipta LestariwahyunurrizkyNo ratings yet
- Alfrex Price List 2019Document1 pageAlfrex Price List 2019wahyunurrizkyNo ratings yet
- MODUL PKN KD1. Pelanggaran Nilai-Nilai PancasilaDocument10 pagesMODUL PKN KD1. Pelanggaran Nilai-Nilai PancasilawahyunurrizkyNo ratings yet
- Sop DieselDocument5 pagesSop DieselwahyunurrizkyNo ratings yet
- PH006 - Atk - IpDocument2 pagesPH006 - Atk - IpwahyunurrizkyNo ratings yet
- Contoh File SummaryDocument2 pagesContoh File SummarywahyunurrizkyNo ratings yet
- PT Indoporlen GlovesDocument2 pagesPT Indoporlen GloveswahyunurrizkyNo ratings yet