You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Contrast Induced NefropathyDocument24 pagesContrast Induced NefropathyRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Alumni CompressedDocument5 pagesAlumni CompressedRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Perioperative Gastro - M. LuckyDocument28 pagesPerioperative Gastro - M. LuckyRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Hubungan Antara Rasio Osteoprotegerin Pada OaDocument179 pagesHubungan Antara Rasio Osteoprotegerin Pada OaRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Kopapdixviii Semarang - Kontingen Papdi JabarDocument3 pagesKopapdixviii Semarang - Kontingen Papdi JabarRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- A Rare Case Presentation Diagnosing Primary Biliary Cholangitis in A Male Patient With Concomitant Type 1 DiabetesDocument8 pagesA Rare Case Presentation Diagnosing Primary Biliary Cholangitis in A Male Patient With Concomitant Type 1 DiabetesRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Skin Disorder PBCDocument6 pagesSkin Disorder PBCRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Diky RamlanDocument10 pagesDiky RamlanRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Referat Advanced Heart FailureDocument21 pagesReferat Advanced Heart FailureRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Favipiravir Versus Other Antiviral or Standard of Care For COVID-19 Treatment: A Rapid Systematic Review and Meta-AnalysisDocument15 pagesFavipiravir Versus Other Antiviral or Standard of Care For COVID-19 Treatment: A Rapid Systematic Review and Meta-AnalysisRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Abstrak WindiDocument15 pagesAbstrak WindiRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Penggunaan High Flow Nasal Cannule Pada Pasien Covid-19Document25 pagesPenggunaan High Flow Nasal Cannule Pada Pasien Covid-19Ratusweethella Intan Yudagrahania PuspitaNo ratings yet
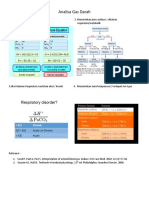
- AGD Rangkuman PDFDocument1 pageAGD Rangkuman PDFRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Tatalaksana DM HT DislipidemiaDocument17 pagesTatalaksana DM HT DislipidemiaRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Tinjauan Pustaka IeDocument6 pagesTinjauan Pustaka IeRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Ensefalitis PsikosisDocument8 pagesEnsefalitis PsikosisRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Case Report Psoriasis Vulgaris Dengan Komplikasi Psoriasis ArtritisDocument39 pagesCase Report Psoriasis Vulgaris Dengan Komplikasi Psoriasis ArtritisRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Word Transfusi DarahDocument25 pagesWord Transfusi DarahRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Bimbingan PatklinDocument15 pagesBimbingan PatklinRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Sumbatan Jalan Nafas Akibat Benda AsingDocument7 pagesSumbatan Jalan Nafas Akibat Benda AsingRatusweethella Intan Yudagrahania PuspitaNo ratings yet