You might also like
- Form Pain DetectDocument2 pagesForm Pain Detectalvin100% (4)
- Revised Log in FormDocument2 pagesRevised Log in FormQueennie Mae LegadaNo ratings yet
- Office Personnel: Department of EducationDocument2 pagesOffice Personnel: Department of EducationCatherine Caluste AlipatNo ratings yet
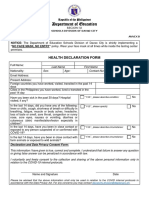
- Health Declaration FormDocument2 pagesHealth Declaration Formbalasan firestationNo ratings yet
- Health Declaration Form: Respondent InformationDocument2 pagesHealth Declaration Form: Respondent Informationmyzzle mendarosNo ratings yet
- Bismonte, Gerald 2. Cantar, Ervin 3. Cantar, Kean 4. Raposon, John Derrick 5. Raposon, Pejay 6. Resare, Daryl 7. Robledo, JonasDocument4 pagesBismonte, Gerald 2. Cantar, Ervin 3. Cantar, Kean 4. Raposon, John Derrick 5. Raposon, Pejay 6. Resare, Daryl 7. Robledo, JonasMARICSON TEOPENo ratings yet
- Learner's Progress ChartDocument4 pagesLearner's Progress ChartRoland PalacioNo ratings yet
- Health Inspection Examination Record.2019Document9 pagesHealth Inspection Examination Record.2019Quennie Edisan MigabonNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesGraceEstoleCaloNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formernesto SumandangNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormLemuel KimNo ratings yet
- Triage Check Up Process FlowDocument3 pagesTriage Check Up Process FlowGlenn Erickson BastoNo ratings yet
- Department of Education Grade 12 TVL: JULY 6, 2022Document2 pagesDepartment of Education Grade 12 TVL: JULY 6, 2022SHAIRUZ DUGAYNo ratings yet
- DCP - Certificate of AppearanceDocument2 pagesDCP - Certificate of AppearanceRobel Monteza CorderoNo ratings yet
- House of Representatives: Student Government of Dumaguete City IDocument2 pagesHouse of Representatives: Student Government of Dumaguete City IKyll Benitez AcademiaNo ratings yet
- GRACE - LABO-COMMUNCATION-FORMAT-2020-longDocument2 pagesGRACE - LABO-COMMUNCATION-FORMAT-2020-longGRACE COLCOLNo ratings yet
- Health Declaration FormDocument3 pagesHealth Declaration FormLESLIE ANN ESTORNINOSNo ratings yet
- 2020 05 22 - 684496o PDFDocument2 pages2020 05 22 - 684496o PDFJessabel Loterte DaoNo ratings yet
- Student Enrolment Application.v1.7Document5 pagesStudent Enrolment Application.v1.7me.madagascarNo ratings yet
- REVISED-LOG-IN-FORM Lumbo ES - Grade 1, 2022-2023 (HEALTH DECLARATION SHEET)Document1 pageREVISED-LOG-IN-FORM Lumbo ES - Grade 1, 2022-2023 (HEALTH DECLARATION SHEET)Novi Joy CatotalNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration FormYanna AbarquezNo ratings yet
- Health LogsheetDocument2 pagesHealth LogsheetRosita DiazNo ratings yet
- Republic of The Philippines Department of Education Region VII - Central VisayasDocument5 pagesRepublic of The Philippines Department of Education Region VII - Central VisayasHyacinth Eiram AmahanCarumba LagahidNo ratings yet
- Alternative Learning System Form - AF2 - Modified ALS Enrolment Form 1Document3 pagesAlternative Learning System Form - AF2 - Modified ALS Enrolment Form 1juniferNo ratings yet
- Athletes e FormsDocument18 pagesAthletes e FormsChristian ALNo ratings yet
- Orca Share Media1585448854138 PDFDocument2 pagesOrca Share Media1585448854138 PDFJopit Olavario RiveraNo ratings yet
- Cennr 2023 1Document1 pageCennr 2023 1Micah MaderajeNo ratings yet
- PMR Employment Application Form. EDMONDDocument5 pagesPMR Employment Application Form. EDMONDEdmond EddieNo ratings yet
- Health Form 3Document2 pagesHealth Form 3Imneil Jeanne PerezNo ratings yet
- Get To Know YouDocument1 pageGet To Know Youapi-371829827No ratings yet
- Department of Education: JULY 7, 2022 Grade 10 EncouragementDocument4 pagesDepartment of Education: JULY 7, 2022 Grade 10 EncouragementSHAIRUZ DUGAYNo ratings yet
- Alfeco Bursary Application Form 1 - (1)Document5 pagesAlfeco Bursary Application Form 1 - (1)Mondli KhothaNo ratings yet
- Department of Education Grade 10 Lavoisier: JULY 7, 2022Document4 pagesDepartment of Education Grade 10 Lavoisier: JULY 7, 2022SHAIRUZ DUGAYNo ratings yet
- Republic Ofthephilippines Region Iv-A CalabarzonDocument2 pagesRepublic Ofthephilippines Region Iv-A Calabarzonsweetheart barrionNo ratings yet
- Application FormDocument2 pagesApplication FormBernard Vincent Guitan MineroNo ratings yet
- Forms Mem - Form Registration Form Copy (Repaired)Document4 pagesForms Mem - Form Registration Form Copy (Repaired)Maria Conxedes GudesNo ratings yet
- Department of Education: Health Declaration FormDocument2 pagesDepartment of Education: Health Declaration FormMaysie BiraquitNo ratings yet
- SHN Form 001 School Health Examination Card ElementaryDocument2 pagesSHN Form 001 School Health Examination Card ElementaryJohn BunayNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormResame ArochaNo ratings yet
- Health Declaration SheetDocument4 pagesHealth Declaration SheetSharon BakerNo ratings yet
- Department of Education: Republic of The PhilippinesDocument5 pagesDepartment of Education: Republic of The PhilippinesCherry Lyn BelgiraNo ratings yet
- Department of Education Schools Division of QuirinoDocument1 pageDepartment of Education Schools Division of QuirinoCyrus AguinaldoNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesAbarra MichelleNo ratings yet
- Retirement Certifications TemplateDocument5 pagesRetirement Certifications TemplateRyan Bornales OcielNo ratings yet
- Deped Region X Community Mapping Template: Enclosure 1Document1 pageDeped Region X Community Mapping Template: Enclosure 1Christine Melody MaramaraNo ratings yet
- Student Individual Inventory: Pangasinan Division Ii Bautista National High SchoolDocument2 pagesStudent Individual Inventory: Pangasinan Division Ii Bautista National High SchoolMichael JunioNo ratings yet
- Enrolment Form-Final 095019Document1 pageEnrolment Form-Final 095019Jade LumantasNo ratings yet
- Enc Encoded SGQGMCVPKDB Fn5a5 tG2ZGpstncf9P9zwaoqfb7dMRlwKjBLAOioftCUGwDocument3 pagesEnc Encoded SGQGMCVPKDB Fn5a5 tG2ZGpstncf9P9zwaoqfb7dMRlwKjBLAOioftCUGwMJ Cortez PaguioNo ratings yet
- RAF Febie PDFDocument1 pageRAF Febie PDFFebie Cleni ArevaloNo ratings yet
- Registration Formdcc 2Document2 pagesRegistration Formdcc 2Emma DionedaNo ratings yet
- Date Accomplished (Signature Over Printed Name) : Evaluated/Processed byDocument2 pagesDate Accomplished (Signature Over Printed Name) : Evaluated/Processed byBello EvenNo ratings yet
- Department of Education Grade 12 Gas: JULY 6, 2022Document3 pagesDepartment of Education Grade 12 Gas: JULY 6, 2022SHAIRUZ DUGAYNo ratings yet
- Form14 - (Name) - (Position) - Application FormDocument4 pagesForm14 - (Name) - (Position) - Application FormBang onad CreatorNo ratings yet
- Child Intake FormDocument4 pagesChild Intake Formapi-544574667No ratings yet
- Department of Education: Learners Profile For The Implementation of Face To Face Classes S.Y. 2021-2022Document5 pagesDepartment of Education: Learners Profile For The Implementation of Face To Face Classes S.Y. 2021-2022Sunghoonieee ParkNo ratings yet
- Po1 Recruitment Application Form: Gonsay Jonathan Binwag P-3 Gabriela Silang, DIFFUN, QUIRINO, Region II 3401Document1 pagePo1 Recruitment Application Form: Gonsay Jonathan Binwag P-3 Gabriela Silang, DIFFUN, QUIRINO, Region II 3401Hahak DougNo ratings yet
- UB Financial ProceduresDocument4 pagesUB Financial ProcedureskhulysimzaNo ratings yet
- Membership Form: Youth For Environment in Schools Organization (Yes-O)Document2 pagesMembership Form: Youth For Environment in Schools Organization (Yes-O)Lurene ReyesNo ratings yet
- Date Accomplished (Signature Over Printed Name) : 1. CitizenshipDocument2 pagesDate Accomplished (Signature Over Printed Name) : 1. CitizenshipJansen TanNo ratings yet
- Bek Kelompok 1Document19 pagesBek Kelompok 1kiranaNo ratings yet
- General Anathesia MSCDocument48 pagesGeneral Anathesia MSCNahla OthmanNo ratings yet
- Laporan Pratikum Farmakoterapi IIDocument3 pagesLaporan Pratikum Farmakoterapi IIniputusukma deviNo ratings yet
- Definiciones en El Marco de Trabajo Del IDDSI de Líquidos y SólidosDocument20 pagesDefiniciones en El Marco de Trabajo Del IDDSI de Líquidos y SólidosLaura IzquierdoNo ratings yet
- Tarana PPT On Trigeminal NeuralgiaDocument37 pagesTarana PPT On Trigeminal NeuralgiaMrinmayee ThakurNo ratings yet
- Tramadol SCDocument5 pagesTramadol SCIzaak AraujoNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaAhmad M AlimNo ratings yet
- Pref - 7 - Vocabulary 3.7 - Revisión Del Intento PDFDocument4 pagesPref - 7 - Vocabulary 3.7 - Revisión Del Intento PDFnaslyNo ratings yet
- Hepatomegaly 1Document5 pagesHepatomegaly 1Bobby ParksNo ratings yet
- Dehydration QuizDocument1 pageDehydration QuizHollie BakerNo ratings yet
- Annex E - COVID 19 Monitoring Tools - v3 Final - 09 23 21Document18 pagesAnnex E - COVID 19 Monitoring Tools - v3 Final - 09 23 21Lovely Mae Madali-BalbuenaNo ratings yet
- Pre-Extern Tutorial, 12Document55 pagesPre-Extern Tutorial, 12Surat TanprawateNo ratings yet
- Trigeminal Autonomic CephalgiasDocument15 pagesTrigeminal Autonomic Cephalgiasheni taridaNo ratings yet
- Chronic Paroxysmal Hemicrania Neurological-Conditions/chronic-Paroxysmal-Hemicrania)Document2 pagesChronic Paroxysmal Hemicrania Neurological-Conditions/chronic-Paroxysmal-Hemicrania)fitriaNo ratings yet
- Aches and Pains VocabularyDocument2 pagesAches and Pains Vocabularystem730% (1)
- It 2 - Signs and Symptoms of Git DisordersDocument54 pagesIt 2 - Signs and Symptoms of Git Disorderspikaanisa100% (9)
- Management of Ardhavabhedaka - A Case ReportDocument4 pagesManagement of Ardhavabhedaka - A Case ReportEditor IJTSRDNo ratings yet
- Case Study For Diagnosis of DiseaseDocument29 pagesCase Study For Diagnosis of DiseaseFirifan DiribaNo ratings yet
- Infus DCDocument216 pagesInfus DCutami kembarNo ratings yet
- Nausea Vomiting ReportDocument67 pagesNausea Vomiting Reportstephanie gayetaNo ratings yet
- The International Classification of Headache Disorders 3rd Edition 2018Document211 pagesThe International Classification of Headache Disorders 3rd Edition 2018Carlos JorgeNo ratings yet
- Declaration Health ChecklistsDocument1 pageDeclaration Health ChecklistsRollie MimisNo ratings yet
- Intro AnesthesiaDocument11 pagesIntro AnesthesiaIffa Aulia HakimNo ratings yet
- Savemom Pregnant Women 1st ScreeningDocument15 pagesSavemom Pregnant Women 1st ScreeningJereeNo ratings yet
- Medical Report Zoe CornelisDocument2 pagesMedical Report Zoe CornelisMuzni RahmanNo ratings yet
- 300 Spartan Medication EbookletDocument201 pages300 Spartan Medication EbookletSVPSNo ratings yet
- Oriented History TakingDocument77 pagesOriented History Takingali laftaNo ratings yet
- Script Bedside Shift ReportDocument2 pagesScript Bedside Shift Report8lueCzarcasmNo ratings yet
- 6 Essential Oils For Nausea - Dr. AxeDocument5 pages6 Essential Oils For Nausea - Dr. AxeJoseph TupasNo ratings yet