You might also like
- Fittp and Red FlagsDocument2 pagesFittp and Red FlagsClaire Madriaga GidoNo ratings yet
- Animal Characters Primitive or DerivedDocument6 pagesAnimal Characters Primitive or DerivedClaire Madriaga GidoNo ratings yet
- Drug Study - HALDOL - ClaireDocument2 pagesDrug Study - HALDOL - ClaireClaire Madriaga GidoNo ratings yet
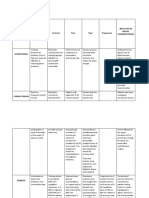
- Medical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsDocument4 pagesMedical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsClaire Madriaga GidoNo ratings yet
- Anatomy and Physiology LabaratoryDocument2 pagesAnatomy and Physiology LabaratoryClaire Madriaga GidoNo ratings yet
- Anatomy and Physiology LabaratoryDocument2 pagesAnatomy and Physiology LabaratoryClaire Madriaga GidoNo ratings yet
- WORKIMMERDocument7 pagesWORKIMMERClaire Madriaga GidoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ebook Current Medical Diagnosis and Treatment 2021 PDF Full Chapter PDFDocument67 pagesEbook Current Medical Diagnosis and Treatment 2021 PDF Full Chapter PDFbeth.hao417100% (27)
- Consolidated List of NDMC HospitalDocument12 pagesConsolidated List of NDMC HospitalgargatworkNo ratings yet
- 25.lower Limb ProstheticsDocument24 pages25.lower Limb ProstheticsThomas Walker100% (1)
- Rubric For Performing Fundal Height MeasurementDocument5 pagesRubric For Performing Fundal Height MeasurementPATRICIA JULIANNE CASTAÑETO RIVERANo ratings yet
- Pediatric AcupunctureDocument11 pagesPediatric AcupunctureAli ElHadi MarmarNo ratings yet
- Astro Diagnosis ScorpioDocument20 pagesAstro Diagnosis ScorpioOvn MurthyNo ratings yet
- Pterygium: By: Ira Rahmawati Universitas Trisakti Jakarta 2013Document16 pagesPterygium: By: Ira Rahmawati Universitas Trisakti Jakarta 2013Ira Rahmawati SigitNo ratings yet
- Claire La Chapelle Complete PDFDocument244 pagesClaire La Chapelle Complete PDFhuyenthanh1807No ratings yet
- Oral Histology NotesDocument18 pagesOral Histology NotesKhalil Raziq100% (1)
- 2019 May List of Physicians and HospitalsDocument7 pages2019 May List of Physicians and HospitalsMuhammad Imteaz AliNo ratings yet
- Chapt 27 Ap2Document5 pagesChapt 27 Ap2candybio83No ratings yet
- OSCE Surgery LatestDocument97 pagesOSCE Surgery LatestPrasad Hewawasam0% (1)
- 432-MI2136 - ESNEFT Clinical Research Fellow (Spec Reg) IpswichDocument15 pages432-MI2136 - ESNEFT Clinical Research Fellow (Spec Reg) IpswichSaquib MohdNo ratings yet
- Nursing Rounds Article PDFDocument13 pagesNursing Rounds Article PDFsuharyaniNo ratings yet
- Febrile SeizuresDocument11 pagesFebrile SeizuresLita Al AmudiNo ratings yet
- Factors Affecting Labor.Document2 pagesFactors Affecting Labor.Salman KhanNo ratings yet
- Ateneo de Zamboanga UniversityDocument3 pagesAteneo de Zamboanga UniversityJuries BintNo ratings yet
- Cerame, Clarisse B. - Uterine Inversion Nursing JournalDocument3 pagesCerame, Clarisse B. - Uterine Inversion Nursing JournalClarisse Biagtan CerameNo ratings yet
- 8699 36053 1 PBDocument7 pages8699 36053 1 PBPatrick RamosNo ratings yet
- Osteogenesis ImperfectaDocument6 pagesOsteogenesis ImperfectaWirahadi SanjayaNo ratings yet
- DR Manish Raval - Varicose Vein Specialist in Rajasthan, Vascular Surgeon in India, BarodaDocument4 pagesDR Manish Raval - Varicose Vein Specialist in Rajasthan, Vascular Surgeon in India, BarodaDr Manish Raval Vascular SurgeonNo ratings yet
- Glasgow Coma Scale GCSDocument4 pagesGlasgow Coma Scale GCScardiacanesthesiaNo ratings yet
- Tugas Percakapan Bahasa Inggris (Kebidanan)Document3 pagesTugas Percakapan Bahasa Inggris (Kebidanan)Elysa WahyuNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Chief Complaint: IndependentDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Chief Complaint: IndependentTed Cipriano VistaNo ratings yet
- Residency Programs Information Sheet 1 AutosavedDocument53 pagesResidency Programs Information Sheet 1 AutosavedPeter Paul PascualNo ratings yet
- Surgical Anatomy PF PNSDocument11 pagesSurgical Anatomy PF PNSdrrahulsshindeNo ratings yet
- 9q Deletions Including 9q33 FTNPDocument10 pages9q Deletions Including 9q33 FTNPMartin GirardNo ratings yet
- Neurosurgical Operative Atlas Volume 1Document471 pagesNeurosurgical Operative Atlas Volume 1bodeadumitru9261100% (7)
- Cervical PolypDocument3 pagesCervical PolypLiyona RifaniNo ratings yet
- QRST CV!!!Document4 pagesQRST CV!!!Menaliza TomasNo ratings yet