You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Wilson - Cranial NervesDocument243 pagesWilson - Cranial NervesBiblioteca CSNT100% (13)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Kitchen Science For Kids PDFDocument40 pagesKitchen Science For Kids PDFimas widowati0% (1)
- CW MELC1 LRv2Document33 pagesCW MELC1 LRv2Lourd Ian Lirazan100% (1)
- Flavour Academy Presentation 2019Document187 pagesFlavour Academy Presentation 2019datdcb100% (1)
- Sensory Evaluation of FoodDocument25 pagesSensory Evaluation of FoodG.p.Aiyer0% (1)
- Word Association Test Manual PDFDocument4 pagesWord Association Test Manual PDFDilawaiz Rasheed0% (3)
- Pranic LifestyleDocument147 pagesPranic LifestyleBoonyarit Huang100% (2)
- Olga Bogdashina-Sensory Perceptual Issues in Autism and Asperger Syndrome - Different Sensory Experiences, Different Perceptual Worlds (2003) PDFDocument219 pagesOlga Bogdashina-Sensory Perceptual Issues in Autism and Asperger Syndrome - Different Sensory Experiences, Different Perceptual Worlds (2003) PDFAlexandra Adda100% (4)
- Studies in The Psychology of Sex, Volume 4 Sexual Selection in Man by Ellis, Havelock, 1859-1939Document187 pagesStudies in The Psychology of Sex, Volume 4 Sexual Selection in Man by Ellis, Havelock, 1859-1939Gutenberg.org100% (5)
- (Handbook of Sensory Physiology 4 - 1 - Chemical Senses.) J. E. Amoore, M. G. J. Beets, J. T. Davies, T. Engen, J. Garcia, R. C. Gesteland, P. P. C. Graziadei, K.-E. Kaissling, R. A. Koelling, J. LeMaDocument542 pages(Handbook of Sensory Physiology 4 - 1 - Chemical Senses.) J. E. Amoore, M. G. J. Beets, J. T. Davies, T. Engen, J. Garcia, R. C. Gesteland, P. P. C. Graziadei, K.-E. Kaissling, R. A. Koelling, J. LeMaArturSobenkoHatumNo ratings yet
- Plaintiffs,: Plaintiff'S Original Petition and Jury DemandDocument8 pagesPlaintiffs,: Plaintiff'S Original Petition and Jury DemandSpectrum NewsNo ratings yet
- Galveston Council December 29 Mardi GRasDocument3 pagesGalveston Council December 29 Mardi GRasSpectrum NewsNo ratings yet
- COVID Gating v1120Document1 pageCOVID Gating v1120Spectrum NewsNo ratings yet
- Amber Alert FlyerDocument1 pageAmber Alert FlyerSpectrum NewsNo ratings yet
- Dallas Police Department Final After Action ReportDocument85 pagesDallas Police Department Final After Action ReportgoodmoineNo ratings yet
- Gov. Greg Abbott's Executive Order Relating To Hospital Capacity During The COVID-9 CrisisDocument4 pagesGov. Greg Abbott's Executive Order Relating To Hospital Capacity During The COVID-9 CrisisRebecca Salinas100% (1)
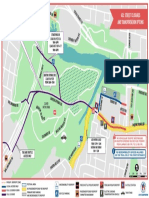
- ACL Zilker Area Map Street Closures Final EnglishDocument1 pageACL Zilker Area Map Street Closures Final EnglishSpectrum NewsNo ratings yet
- Stay Home Work Safe OrderDocument15 pagesStay Home Work Safe OrderCBS Austin Webteam100% (4)
- Bike Lanes Lower BrdwyDocument10 pagesBike Lanes Lower BrdwySpectrum NewsNo ratings yet
- Tuesday, September 24, 2019: Special Thanks To Our Affiliate Service ProvidersDocument8 pagesTuesday, September 24, 2019: Special Thanks To Our Affiliate Service ProvidersSpectrum NewsNo ratings yet
- Tuesday, September 24, 2019: Special Thanks To Our Affiliate Service ProvidersDocument8 pagesTuesday, September 24, 2019: Special Thanks To Our Affiliate Service ProvidersSpectrum NewsNo ratings yet
- pr1 PDFDocument137 pagespr1 PDFSiegrid Anne TamayoNo ratings yet
- Unit 5. Interaction and HealthDocument11 pagesUnit 5. Interaction and Healthtamarita90No ratings yet
- Analyzing The Impact of Sensory Marketing On Consumers: A Case Study of KFCDocument15 pagesAnalyzing The Impact of Sensory Marketing On Consumers: A Case Study of KFCArpit JainNo ratings yet
- Luigi Toiati - SinestesiaDocument6 pagesLuigi Toiati - Sinestesiasergio_poblete_ortegaNo ratings yet
- Libro Analisis Sensorial - VinosDocument35 pagesLibro Analisis Sensorial - VinosNAYBEANo ratings yet
- Origins of Objectivity - Reviews - Notre Dame Philosophical Reviews - University of Notre DameDocument23 pagesOrigins of Objectivity - Reviews - Notre Dame Philosophical Reviews - University of Notre DameKesia RamosNo ratings yet
- Placement TestDocument10 pagesPlacement TestFathy ElsheshtawyNo ratings yet
- FINAL 2017 Ures ProgramDocument77 pagesFINAL 2017 Ures ProgramPatrick Matthew GreenNo ratings yet
- Module No. 2Document7 pagesModule No. 2Zarah CaloNo ratings yet
- Anatomy Ch. 9 The Senses NotesDocument7 pagesAnatomy Ch. 9 The Senses Notesprincepalestine100% (1)
- The Five SensesDocument4 pagesThe Five SensesMadalina CiurdeaNo ratings yet
- Science Magazine 5694 2004-10-08 PDFDocument89 pagesScience Magazine 5694 2004-10-08 PDFTân ChipNo ratings yet
- SAPS - Using Your Nose - Smell ActivitiesDocument11 pagesSAPS - Using Your Nose - Smell ActivitiesMichael Restrepo GarciaNo ratings yet
- OlfactionDocument18 pagesOlfactionsuderson100% (1)
- A Cognitive Experimental Approach To Understanding and Reducing Food CravingsDocument5 pagesA Cognitive Experimental Approach To Understanding and Reducing Food CravingsyodoidNo ratings yet
- Finalcopy q1w1 Oralcomm SalvadorDocument10 pagesFinalcopy q1w1 Oralcomm SalvadorLorie-Lyn De Guzman SalvadorNo ratings yet
- Gan, Ryan Elbert Z. GsflaedDocument34 pagesGan, Ryan Elbert Z. GsflaedRyan Elbert Zabala GanNo ratings yet
- Creative WritingDocument3 pagesCreative WritingRee April CabalanNo ratings yet
- Nervus Olfaktorius: Dasar, Klinis Medis, Dan Psikologis: Pingkan Ruru, Taufiq Fredrik Pasiak, Martha Marie KasekeDocument9 pagesNervus Olfaktorius: Dasar, Klinis Medis, Dan Psikologis: Pingkan Ruru, Taufiq Fredrik Pasiak, Martha Marie KasekeAfsarDwiNo ratings yet
- Astm e 619 - 84 R03Document5 pagesAstm e 619 - 84 R03Francisco GuerraNo ratings yet