You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
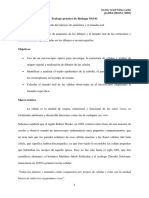
- Trabajo Práctico de Biología NM #1 - Cálculo Del Número de Aumentos y El Tamaño Real.Document16 pagesTrabajo Práctico de Biología NM #1 - Cálculo Del Número de Aumentos y El Tamaño Real.Jeremy Palma86% (21)
- CHNDocument340 pagesCHNPao ParelNo ratings yet
- Matriz de Identificación de Peligros Supermercado CundiDocument2 pagesMatriz de Identificación de Peligros Supermercado CundiAndresFelipeQuinteroDaza93% (14)
- %RSD Atau CV SD/Mean×100%Document2 pages%RSD Atau CV SD/Mean×100%Futna NaufaNo ratings yet
- Tidur Larut MalamDocument2 pagesTidur Larut MalamFutna NaufaNo ratings yet
- B IndonesiaDocument2 pagesB IndonesiaFutna Naufa50% (2)
- Euphorbia Hirta (Patikan Kebo)Document6 pagesEuphorbia Hirta (Patikan Kebo)Futna NaufaNo ratings yet
- Euphorbia Hirta (Patikan Kebo)Document6 pagesEuphorbia Hirta (Patikan Kebo)Futna NaufaNo ratings yet
- Modelo de AnamneseDocument24 pagesModelo de Anamnesetalita juliaNo ratings yet
- Bperit Template - CópiaDocument31 pagesBperit Template - CópiaJorge DärwenNo ratings yet
- Accidente Cerebrovascular: Medicina Interna InternadoDocument56 pagesAccidente Cerebrovascular: Medicina Interna InternadoMaría José TilleriaNo ratings yet
- Discrepancia ABO UPLADocument16 pagesDiscrepancia ABO UPLAMARY0% (1)
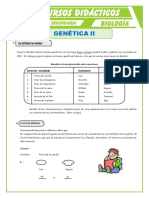
- Genética Ii: Los Estudios de MendelDocument4 pagesGenética Ii: Los Estudios de MendelPe Rro Enmoscado100% (1)
- Nursing Process Septate UterusDocument6 pagesNursing Process Septate UterusJay PaulNo ratings yet
- Rapport Projet TutoréDocument6 pagesRapport Projet TutoréÉmile Kwamo100% (1)
- Chapter-2 RRLDocument98 pagesChapter-2 RRLLovlegin DiongNo ratings yet
- Thesis Statement Examples Air PollutionDocument8 pagesThesis Statement Examples Air Pollutionmistygordonarlington100% (2)
- Programa de Estilos de Vida SaludableDocument22 pagesPrograma de Estilos de Vida SaludableFrancisco Torres FuentesNo ratings yet
- Centro de Cirugia AmbulatoriaDocument61 pagesCentro de Cirugia AmbulatoriaLeoSilva100% (3)
- Cuestionario Gastro EndocrinoDocument5 pagesCuestionario Gastro EndocrinoSebastianNo ratings yet
- CTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongDocument33 pagesCTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongSabrina AzizNo ratings yet
- Distocia de Presentación CefálicaDocument30 pagesDistocia de Presentación CefálicaRodriguez Pao67% (3)
- Nefrotoxicidad de CefalosporinasDocument2 pagesNefrotoxicidad de CefalosporinasCdcgs PWinNo ratings yet
- Methylphenidate (Ritalin) - Associated Cataract and GlaucomaDocument2 pagesMethylphenidate (Ritalin) - Associated Cataract and GlaucomaMohamad Nazrin YahayaNo ratings yet
- Consentimiento Informado LipoesculturaDocument6 pagesConsentimiento Informado LipoesculturaMiguel RojNo ratings yet
- Quantum TouchDocument4 pagesQuantum Touchvaleska27No ratings yet
- AracnoidesDocument11 pagesAracnoidesJesus Smaikel Teran MuenalaNo ratings yet
- Kekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode AsteriknyaDocument3 pagesKekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode Asteriknyaarachis arumawatiNo ratings yet
- 5 - VerminosesDocument13 pages5 - VerminosesIsabella Novaes100% (2)
- Resumo Vias Aferentes Medulares - Dor e TemperaturaDocument3 pagesResumo Vias Aferentes Medulares - Dor e TemperaturaIsabella Nino100% (1)
- Triptico de La OcaDocument2 pagesTriptico de La OcaFèlix Salazar Ludeña100% (1)
- Physiologie Du ReinDocument15 pagesPhysiologie Du Reinntoutoumelucas17No ratings yet
- Tesis - Ascencio DiosesDocument81 pagesTesis - Ascencio Dioseswilson DuarteNo ratings yet
- Reacciones FebrilesDocument14 pagesReacciones FebrilesLa Diva Diva0% (1)
- Barriers and Facilitators That Influence Telemedicine Based Real Time, Online Consultation at Patients Homes Systematic Literature ReviewDocument25 pagesBarriers and Facilitators That Influence Telemedicine Based Real Time, Online Consultation at Patients Homes Systematic Literature ReviewLupe sifuentes martinezNo ratings yet