You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Metal Gear Solid - Characters Profile and TimelineDocument65 pagesMetal Gear Solid - Characters Profile and Timelinekrevorkian1653100% (1)
- Steel Forgings, Carbon and Alloy, For Pinions, Gears and Shafts For Reduction GearsDocument4 pagesSteel Forgings, Carbon and Alloy, For Pinions, Gears and Shafts For Reduction Gearssharon blushteinNo ratings yet
- Assimil Brazilian Portuguese (Portuguese Edition)Document15 pagesAssimil Brazilian Portuguese (Portuguese Edition)robertocarmur43% (23)
- Sir Syed Ahmed Khan and Two Nation TheoryDocument11 pagesSir Syed Ahmed Khan and Two Nation TheoryZeeshan Saeed100% (5)
- Albert Szent-Gyorgyi-The Scientist Who DiscoveredDocument8 pagesAlbert Szent-Gyorgyi-The Scientist Who DiscoveredCristina ElenaNo ratings yet
- Virgin Galactic Profile & Performance Business ReportDocument10 pagesVirgin Galactic Profile & Performance Business ReportLoic PitoisNo ratings yet
- Rapid Prototyping and ToolingDocument2 pagesRapid Prototyping and ToolingelangandhiNo ratings yet
- Construction ProjectsDocument13 pagesConstruction ProjectsMuhammad SafdarNo ratings yet
- Engel King 2015Document6 pagesEngel King 2015Cristina ElenaNo ratings yet
- Effect of Vitamin C Intake On Human HealthDocument13 pagesEffect of Vitamin C Intake On Human HealthCristina ElenaNo ratings yet
- Baqai J Health Sci 2011 14 2 33 40Document8 pagesBaqai J Health Sci 2011 14 2 33 40Cristina ElenaNo ratings yet
- Donor de eDocument7 pagesDonor de eCristina ElenaNo ratings yet
- A.I.1. Derivati de Adamantan: Amantadina.: A. Medicamente Indicate in Infectii Virale RespiratoriiDocument42 pagesA.I.1. Derivati de Adamantan: Amantadina.: A. Medicamente Indicate in Infectii Virale RespiratoriiCristina ElenaNo ratings yet
- Activity Sheets Q1 - SVADocument5 pagesActivity Sheets Q1 - SVAAlma ReynaldoNo ratings yet
- STEPOSOLMET10 UHousehold Cleaning Sales ToolDocument2 pagesSTEPOSOLMET10 UHousehold Cleaning Sales Toolpkh29No ratings yet
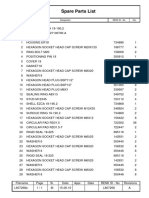
- L807268EDocument1 pageL807268EsjsshipNo ratings yet
- Have To, Has To, Had To - Exercise 1 - Worksheet English GrammarDocument1 pageHave To, Has To, Had To - Exercise 1 - Worksheet English Grammarjonni jonsonNo ratings yet
- Cedarwood ChromatographyDocument6 pagesCedarwood ChromatographyMartinaNo ratings yet
- Analogy - 10 Page - 01 PDFDocument10 pagesAnalogy - 10 Page - 01 PDFrifathasan13No ratings yet
- Reynald Hernandez: ExperienceDocument2 pagesReynald Hernandez: ExperienceRey HernandezNo ratings yet
- Excel Subhadip NandyDocument9 pagesExcel Subhadip NandyNihilisticDelusionNo ratings yet
- Neonatal Phototherapy: Operator ManualDocument16 pagesNeonatal Phototherapy: Operator ManualAbel FencerNo ratings yet
- Formalismo Geométrico de La Mecánica Cuántica y Sus Aplicaciones A Modelos MolecularesDocument51 pagesFormalismo Geométrico de La Mecánica Cuántica y Sus Aplicaciones A Modelos Moleculareshugo_valles_2No ratings yet
- 6.1 Mean Median Mode and RangeDocument21 pages6.1 Mean Median Mode and RangeGilbert Guzman TurarayNo ratings yet
- Tripwire Is An Intrusion Detection SystemDocument28 pagesTripwire Is An Intrusion Detection SystempoornimaNo ratings yet
- SDS - Molykote 1000Document8 pagesSDS - Molykote 1000Zarni KyawNo ratings yet
- ReportDocument1 pageReportyousufNo ratings yet
- 24 - Mubangizi-WHOPQP GMP Inspections UpdatesDocument17 pages24 - Mubangizi-WHOPQP GMP Inspections UpdatessamxuNo ratings yet
- Pyneng Readthedocs Io en LatestDocument702 pagesPyneng Readthedocs Io en LatestNgọc Duy VõNo ratings yet
- The Enemy Within - v18Document8 pagesThe Enemy Within - v18Matt WillisNo ratings yet
- Eyu-Ethiopia FinanceOperations Manual January2020 v1 EnglishDocument104 pagesEyu-Ethiopia FinanceOperations Manual January2020 v1 EnglishHenockNo ratings yet
- RK20 Power Flow SparseDocument33 pagesRK20 Power Flow Sparsejohn smithNo ratings yet
- 3 Parts of A Science Fair ProjectDocument5 pages3 Parts of A Science Fair ProjectGeorge Oswald Junior CarringtonNo ratings yet
- Economics Key WordsDocument30 pagesEconomics Key WordsJanetNo ratings yet
- 1 Scrum Master Skills m1 Slides PDFDocument66 pages1 Scrum Master Skills m1 Slides PDFSohaib Omer SalihNo ratings yet
- Module 2 Tssig Week 2 3Document4 pagesModule 2 Tssig Week 2 3Alysa QuintanarNo ratings yet