You might also like
- Open Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective StudyDocument3 pagesOpen Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective Study'Adil MuhammadNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Hernia - Hernioplasty With Bilayer Polypropylene Mesh PDFDocument4 pagesHernia - Hernioplasty With Bilayer Polypropylene Mesh PDFAnonymous YLmmme4XX0No ratings yet
- Treatment: Bassini RepairDocument5 pagesTreatment: Bassini RepairziehonkNo ratings yet
- Incisional HerniaDocument13 pagesIncisional HerniaMaya Dewi permatasariNo ratings yet
- Tension-Free Repair Versus Bassini Technique For SDocument5 pagesTension-Free Repair Versus Bassini Technique For STomus ClaudiuNo ratings yet
- Groin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYDocument39 pagesGroin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYMuhammad Waqar UlfatNo ratings yet
- OP Sliding & Strangulated Hernia & OrchiectomyDocument8 pagesOP Sliding & Strangulated Hernia & OrchiectomyDeepika ChaudharyNo ratings yet
- CA OesophagusDocument47 pagesCA OesophagusAnsif KNo ratings yet
- HernioplastyDocument58 pagesHernioplastyFobin VargheseNo ratings yet
- Essential Techniques for Safe Thyroid SurgeryDocument26 pagesEssential Techniques for Safe Thyroid SurgeryJimmyNo ratings yet
- Mesh MaterialsDocument21 pagesMesh MaterialsbogdanotiNo ratings yet
- Idiopathic Non Neoplastic Salivary Gland DiseasesDocument33 pagesIdiopathic Non Neoplastic Salivary Gland Diseasesgud4nothingNo ratings yet
- SoTM StaplingDocument20 pagesSoTM StaplingIndrawan Buleth100% (1)
- Energy Devices in Surgery: Surg LT CDR K S PatelDocument32 pagesEnergy Devices in Surgery: Surg LT CDR K S PatelMuhammad ShahidNo ratings yet
- Prosthetic Material in Inguinal Hernia RepairDocument23 pagesProsthetic Material in Inguinal Hernia RepairAnca NicaNo ratings yet
- Surgical Meshes and Their FixationDocument34 pagesSurgical Meshes and Their FixationShahzad Alam ShahNo ratings yet
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Principles of Electrosurgery and DiathermyDocument15 pagesPrinciples of Electrosurgery and DiathermyRajarshi KumarNo ratings yet
- Etiopathogenesis & Staging of Cancer BreastDocument25 pagesEtiopathogenesis & Staging of Cancer Breastapi-3701915No ratings yet
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Back To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopDocument43 pagesBack To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopBima Achmad100% (1)
- Hernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsDocument43 pagesHernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsFobin VargheseNo ratings yet
- HerniaDocument16 pagesHerniaVetrivel TamizhNo ratings yet
- Role of neck triangles in identifying structures during thyroid surgeryDocument6 pagesRole of neck triangles in identifying structures during thyroid surgeryJay-arh SebusaNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- The Surgical Anatomy of The Nerve Laryngeal RecurrensDocument2 pagesThe Surgical Anatomy of The Nerve Laryngeal RecurrensvaNo ratings yet
- New Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSDocument21 pagesNew Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSArturo Javier FuentesNo ratings yet
- Premalignant & Malignant Disease of CervixDocument64 pagesPremalignant & Malignant Disease of CervixDegefaw BikoyNo ratings yet
- Motility Disorders of EsophagusDocument44 pagesMotility Disorders of EsophagusmackieccNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Thyroid Disorders: Types, Symptoms, and TreatmentsDocument41 pagesThyroid Disorders: Types, Symptoms, and Treatmentssheila_kohNo ratings yet
- Parotid TumorDocument37 pagesParotid TumorRiyan SaputraNo ratings yet
- What Is The Differential Diagnosis For The Breast Mass in An Adolescent?Document4 pagesWhat Is The Differential Diagnosis For The Breast Mass in An Adolescent?theodore_estradaNo ratings yet
- Neet StuffDocument26 pagesNeet StuffBalasubrahmanya K. R.No ratings yet
- Scrotal SwellingDocument40 pagesScrotal Swellingeirene simbolonNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- Varicose Veins CaseDocument16 pagesVaricose Veins Casebenak shivalingappaNo ratings yet
- VaricoceleDocument19 pagesVaricoceleMariam AntonyNo ratings yet
- 04 Esophageal TumorsDocument36 pages04 Esophageal TumorsDetty NoviantyNo ratings yet
- I Flat Meshes For Inguinal and Ventral Hernias V 2Document30 pagesI Flat Meshes For Inguinal and Ventral Hernias V 2bogdanoti100% (1)
- Blunt Adominal TraumaDocument14 pagesBlunt Adominal TraumaMuhammad Bima AkbarNo ratings yet
- Development of MesentryDocument28 pagesDevelopment of MesentryimmmiNo ratings yet
- Energy Sources in SurgeryDocument68 pagesEnergy Sources in SurgeryKhan Qayyum KhanNo ratings yet
- Penetrating Abdominal TraumaDocument3 pagesPenetrating Abdominal TraumaamrulNo ratings yet
- Rectal Cancer PPT 2.1Document131 pagesRectal Cancer PPT 2.1Usmle GuyNo ratings yet
- Bowel AnastomosisDocument30 pagesBowel AnastomosismrashaiedehNo ratings yet
- Reconstruction in Fournier GangreneDocument40 pagesReconstruction in Fournier GangreneAnggie MutmainnahNo ratings yet
- Carcinoma Oesophagus: Dr. S. Ranita DeviDocument46 pagesCarcinoma Oesophagus: Dr. S. Ranita DeviVivek AhanthemNo ratings yet
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- A Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryDocument9 pagesA Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryJWPlasticsurgeryNo ratings yet
- NCCN HCC For Patients 2020Document76 pagesNCCN HCC For Patients 2020Dona LagurinNo ratings yet
- Surgery of PancreasDocument30 pagesSurgery of PancreasmackieccNo ratings yet
- Malignant Breast DiseasesDocument49 pagesMalignant Breast DiseasesEsha BhatiaNo ratings yet
- A Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressDocument299 pagesA Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressHamza Khan100% (1)
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Hernia Examination SchemeDocument4 pagesHernia Examination Schemeatribecalledquest20No ratings yet
- Abdominal Trauma Assessment GuideDocument135 pagesAbdominal Trauma Assessment GuidewidyastutiNo ratings yet
- LiverDocument27 pagesLiverAndi Arwan AgusnawanNo ratings yet
- Creating Effective Teams Week 11 LessonDocument4 pagesCreating Effective Teams Week 11 LessonEll VNo ratings yet
- Outcome Predictors in Acute Surgical Admissions For Lower Gastrointestinal BleedingDocument1 pageOutcome Predictors in Acute Surgical Admissions For Lower Gastrointestinal BleedingEd FitzgeraldNo ratings yet
- Cynthia Orange - Sing Your Own Song - A Guide For Single Moms-Hazelden (2001) PDFDocument203 pagesCynthia Orange - Sing Your Own Song - A Guide For Single Moms-Hazelden (2001) PDFegalNo ratings yet
- Institución Educativa Almirante Padilla: Informacion Basica de La Secuencia DidacticaDocument3 pagesInstitución Educativa Almirante Padilla: Informacion Basica de La Secuencia DidacticaGreys NarvaezNo ratings yet
- Insurance Claim FormDocument3 pagesInsurance Claim FormAnubhav VardhanNo ratings yet
- Coomber, & Barriball, 2007Document18 pagesCoomber, & Barriball, 20070112joeriNo ratings yet
- Anti-Smoking Barangay ScorecardDocument2 pagesAnti-Smoking Barangay ScorecardBarangay PitaNo ratings yet
- Chap 26 - Assessing Male Genitalia (Interview Guide)Document3 pagesChap 26 - Assessing Male Genitalia (Interview Guide)Mary Cielo DomagasNo ratings yet
- Climbing WorkoutsDocument59 pagesClimbing WorkoutsAlexandre Santos100% (8)
- Position PaperDocument3 pagesPosition PaperlaxmiNo ratings yet
- Assessing The Life Satisfaction of Elderly Living in Old Age Homes in The City of Ahmedabad-28-43Document16 pagesAssessing The Life Satisfaction of Elderly Living in Old Age Homes in The City of Ahmedabad-28-43Nageswara Rao AmbatiNo ratings yet
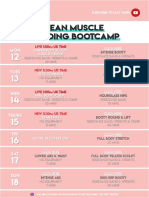
- 26 - LEAN Weekly Guide - On - October 12Document15 pages26 - LEAN Weekly Guide - On - October 12Andrea CsillaNo ratings yet
- Lesson Plan in Bread and Pastry Production Ncii I. ObjectivesDocument2 pagesLesson Plan in Bread and Pastry Production Ncii I. ObjectivesDezzelyn Balleta100% (1)
- ENVS 1301 Learning Guide Unit 1 Discussion Assignment HomeDocument2 pagesENVS 1301 Learning Guide Unit 1 Discussion Assignment HomehomepoetNo ratings yet
- AI Breast ScreeningDocument2 pagesAI Breast ScreeningChan Chee HouNo ratings yet
- Corona Cavach Policy WordingsDocument14 pagesCorona Cavach Policy WordingsRajesh SirsathNo ratings yet
- SS1 English Language Comprehension and Objective QuestionsDocument5 pagesSS1 English Language Comprehension and Objective QuestionsJoshua OshokpekhaNo ratings yet
- Gad PBDocument11 pagesGad PBMary Car Failana FabularumNo ratings yet
- Pre-Intermediate, Chapter 1 Test: Select Readings, Second EditionDocument2 pagesPre-Intermediate, Chapter 1 Test: Select Readings, Second Editionreihaneh azimi100% (1)
- Career and Development CounselingDocument3 pagesCareer and Development CounselingNico PelomianoNo ratings yet
- VSP - Vision 01Document1 pageVSP - Vision 01api-252555369No ratings yet
- Hazard Identification and Risk Assessment for Confined Space WorkDocument4 pagesHazard Identification and Risk Assessment for Confined Space Workaman anand100% (2)
- From Head To ToeDocument5 pagesFrom Head To Toeapi-500025821No ratings yet
- Swamy PDFDocument20 pagesSwamy PDFsreejithNo ratings yet
- Title Lorem IpsumDocument11 pagesTitle Lorem IpsumPrithu YashasNo ratings yet
- Communication Research PaperDocument7 pagesCommunication Research Paperafnknlsjcpanrs100% (1)
- TFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDocument2 pagesTFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDanica Rose PalacaNo ratings yet
- SIA 6 and SPS 6 - English - Copyright - 2017Document1 pageSIA 6 and SPS 6 - English - Copyright - 2017CarolNo ratings yet
- Annual Medical Report Form Annapolis - Ho 2020Document10 pagesAnnual Medical Report Form Annapolis - Ho 2020Melissa DavidNo ratings yet
- 2019 Jerrold The Extraction of Teeth Part 2 Considerations Regarding Which Teeth To Extract Seminars in OrthodonticsDocument9 pages2019 Jerrold The Extraction of Teeth Part 2 Considerations Regarding Which Teeth To Extract Seminars in Orthodonticsplayer osamaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)