You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Original ArticleDocument8 pagesOriginal ArticleCelina Castañeda MartinezNo ratings yet
- PrescriptionDocument18 pagesPrescriptionAlphahin 17No ratings yet
- IJNHDocument6 pagesIJNHMaheboob GanjalNo ratings yet
- CUESDocument2 pagesCUESJhia Dela PeñaNo ratings yet
- IJALIBVol 9no 1june 2018CRC4KabiruDanladiGarbaDocument7 pagesIJALIBVol 9no 1june 2018CRC4KabiruDanladiGarbaGabrielNo ratings yet
- School Health ServicesDocument2 pagesSchool Health ServicesSusan Loida SorianoNo ratings yet
- 2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFDocument14 pages2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFgiseladlrNo ratings yet
- Medical Tourism: A Study of Kerala: Project SynopsisDocument2 pagesMedical Tourism: A Study of Kerala: Project SynopsisbhatiaharryjassiNo ratings yet
- COPARDocument7 pagesCOPARAlexis Trinidad0% (1)
- Burning Mouth Syndrome and Treatment With ParoxetinDocument2 pagesBurning Mouth Syndrome and Treatment With ParoxetinFitri AngginiNo ratings yet
- 5 Measuring Dental FluorosisDocument26 pages5 Measuring Dental Fluorosisashwq9854No ratings yet
- Plastic Surgery Logbook Batch A - EditedDocument11 pagesPlastic Surgery Logbook Batch A - EditedRidham RanaNo ratings yet
- Injuries of The Sporting KneeDocument3 pagesInjuries of The Sporting KneeDanar Hari AdhimuktiNo ratings yet
- Jessica 20jonesDocument2 pagesJessica 20jonesapi-392730765No ratings yet
- AO 2016-0042 Annex H-9a Checklist For Review of Floor Plans - Acute-Chronic Psychiatric Care FacilityDocument3 pagesAO 2016-0042 Annex H-9a Checklist For Review of Floor Plans - Acute-Chronic Psychiatric Care FacilityonnijNo ratings yet
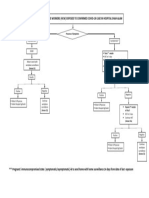
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- IS MI - Transes SkillsDocument5 pagesIS MI - Transes Skillsmaaisley.yebanNo ratings yet
- PRBSEC-47 Internal Examination FormDocument5 pagesPRBSEC-47 Internal Examination FormHasna ButongkayNo ratings yet
- CABG Discharge Planning 1Document16 pagesCABG Discharge Planning 1pipporudyNo ratings yet
- Introduction To Occupational TherapyDocument9 pagesIntroduction To Occupational TherapyDevy CaruzNo ratings yet
- (HEALTH) - Q1 - MODULE 1&2 - FOR COMPETENCY #1to7 - CONSUMER HEALTHV1Document11 pages(HEALTH) - Q1 - MODULE 1&2 - FOR COMPETENCY #1to7 - CONSUMER HEALTHV1Khem SumayloNo ratings yet
- Compre FundaDocument10 pagesCompre FundaAngie SaquingNo ratings yet
- Mazhaume Eugan CVDocument5 pagesMazhaume Eugan CVMaxwell MandikumbaNo ratings yet
- Standar Alat AmbulanceDocument4 pagesStandar Alat AmbulanceDonny LogantaraNo ratings yet
- Safe Work Method Statement (SWMS) Infection Prevention & ControlDocument1 pageSafe Work Method Statement (SWMS) Infection Prevention & ControlAnoirNo ratings yet
- Snapshot NCP Step 3 Nutrition Intervention-1Document1 pageSnapshot NCP Step 3 Nutrition Intervention-1api-250924915No ratings yet
- AOP 2024 Buenavista QuezonDocument270 pagesAOP 2024 Buenavista QuezonChristian Lawrence ReyesNo ratings yet
- Chap 20 LeadershipDocument4 pagesChap 20 LeadershipklossmaddyNo ratings yet
- Paula Monlux Resume 2Document4 pagesPaula Monlux Resume 2Paula Garman MonluxNo ratings yet
- English About PharmacyDocument12 pagesEnglish About PharmacySyamil AdibaNo ratings yet