You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Material Safety Data Sheet Material Safety Data SheetDocument3 pagesMaterial Safety Data Sheet Material Safety Data SheetKarthik0% (2)
- Introduction To Medical SociologyDocument16 pagesIntroduction To Medical SociologyGiorgi JafaridzeNo ratings yet
- Dysmenorrhea Social Support Anxiety Pain LevelsDocument8 pagesDysmenorrhea Social Support Anxiety Pain LevelsEgawidya EgaNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
- Cdmgens00160 PDFDocument111 pagesCdmgens00160 PDFMohammadMasoomParwezNo ratings yet
- Argument Essay Final - Katie Adams 2Document6 pagesArgument Essay Final - Katie Adams 2api-608656301No ratings yet
- Term Paper TitlesDocument6 pagesTerm Paper TitlesGOOD BATA WAY BITOKNo ratings yet
- CSP Chintu Anna - 1Document12 pagesCSP Chintu Anna - 1sujithNo ratings yet
- Batangas State University NSTP Project on Community GardeningDocument17 pagesBatangas State University NSTP Project on Community Gardeningjaerald estiocoNo ratings yet
- Reflective Practice JournalDocument5 pagesReflective Practice JournalReuben RussellNo ratings yet
- Roth - From Free WombDocument19 pagesRoth - From Free WombNubss SSNo ratings yet
- Products Category Pack Size MRP (Inr) : Qnet India Product Price List EFFECTIVE January 1st 2020Document2 pagesProducts Category Pack Size MRP (Inr) : Qnet India Product Price List EFFECTIVE January 1st 2020Gopal SainiNo ratings yet
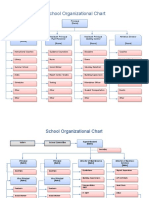
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- Eni North Africa BV WTP Nalue HospitalDocument3 pagesEni North Africa BV WTP Nalue HospitalHedi Ben MohamedNo ratings yet
- Curriculum Vitae: Amir E. Ibrahim, M.DDocument11 pagesCurriculum Vitae: Amir E. Ibrahim, M.DkendoNo ratings yet
- Cozen ResumeDocument3 pagesCozen Resumeapi-534216481No ratings yet
- Helene Deutsch, A Psychoanalysts Life (Lacanempdf)Document400 pagesHelene Deutsch, A Psychoanalysts Life (Lacanempdf)Carlos AugustoNo ratings yet
- COVID vaccination certificate for Indian teenDocument1 pageCOVID vaccination certificate for Indian teenShubham TiwariNo ratings yet
- Physio 2.05 Bloodphysiology2 HemostasisDocument9 pagesPhysio 2.05 Bloodphysiology2 HemostasisSimon Peter Familara100% (1)
- 27 Annual ReportDocument102 pages27 Annual Reportudiptya_papai2007No ratings yet
- IVMS Comprehensive Pathology Examination W AnswersDocument55 pagesIVMS Comprehensive Pathology Examination W AnswersMarc Imhotep Cray, M.D.100% (4)
- HUMAN REPRODUCTION-1 Madhu - QuestionDocument69 pagesHUMAN REPRODUCTION-1 Madhu - QuestionAyan Sarkar100% (1)
- Implementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFDocument22 pagesImplementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFMonica DyerNo ratings yet
- Blue Royale PlanDocument8 pagesBlue Royale PlanMikele Molina BetervoNo ratings yet
- Periprosthetic Joint Infection ISM 2013Document362 pagesPeriprosthetic Joint Infection ISM 2013Andrei Costin100% (1)
- ASCE's Roadmap to Sustainable InfrastructureDocument5 pagesASCE's Roadmap to Sustainable InfrastructureRodolfo De La GarzaNo ratings yet
- Cpale 2022Document3 pagesCpale 2022Mario ErazoNo ratings yet
- Intelligent ConstructionDocument4 pagesIntelligent ConstructionRikesh SapkotaNo ratings yet
- Project On-Law of Torts Topic - NegligenceDocument10 pagesProject On-Law of Torts Topic - NegligenceSoumya Shefali ChandrakarNo ratings yet
- Method Statement For PlasteringDocument14 pagesMethod Statement For Plasteringjameel100% (1)