You might also like
- Quantification of Severity of Mitral Regurgitation With The New ASE GuidelinesDocument20 pagesQuantification of Severity of Mitral Regurgitation With The New ASE GuidelinesPanfilAlinaNo ratings yet
- IgA Nephropathy Burgers Disease Case ReportDocument3 pagesIgA Nephropathy Burgers Disease Case ReportResearch ParkNo ratings yet
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- End Stage Renal Disease Case StudyDocument8 pagesEnd Stage Renal Disease Case StudyNikko Dela CruzNo ratings yet
- Immunoglobulin A Nephropathy: Current UpdatesDocument61 pagesImmunoglobulin A Nephropathy: Current UpdatesRahul PabalkarNo ratings yet
- Warhammer - FB - Converting OgresDocument3 pagesWarhammer - FB - Converting OgresAndy Kirkwood100% (3)
- Targeting Israeli Apartheid Jan 2012Document384 pagesTargeting Israeli Apartheid Jan 2012Pepe SalasNo ratings yet
- Nutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFDocument64 pagesNutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFjvprasad100% (1)
- All The Orbats v1-5-4Document21 pagesAll The Orbats v1-5-4petesqueeler7052No ratings yet
- Dysrhythmia Advance Content Outline A1 - 2020.1.2Document3 pagesDysrhythmia Advance Content Outline A1 - 2020.1.2Kimberly Whiteside50% (2)
- Cardiothoracic Surgery Board ReviewDocument4,053 pagesCardiothoracic Surgery Board ReviewKrishna RajakumarNo ratings yet
- Cardiac ArrhythmiasDocument14 pagesCardiac ArrhythmiasArvin John ManuelNo ratings yet
- Oftal Case StudyDocument11 pagesOftal Case StudyMohamad RaisNo ratings yet
- TX Nefropatia Por IgADocument8 pagesTX Nefropatia Por IgAIsrael Armida SodanargNo ratings yet
- IgA Nephropathy Info SheetDocument2 pagesIgA Nephropathy Info Sheetheba.barkasiehNo ratings yet
- CKD 24 1 1Document13 pagesCKD 24 1 1prisky chriselawatiNo ratings yet
- Iga Nephropathy (Berger'S Disease)Document8 pagesIga Nephropathy (Berger'S Disease)NourNo ratings yet
- Rapidly Progressive IgA Nephropathy Leads To End-Stage Renal Disease A Case ReportDocument3 pagesRapidly Progressive IgA Nephropathy Leads To End-Stage Renal Disease A Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Predictors of Prognosis in Iga Nephropathy: Review ArticleDocument4 pagesPredictors of Prognosis in Iga Nephropathy: Review ArticledavidpuaNo ratings yet
- IgAnephropathy in Adults Treatments Standard NDT 2023Document10 pagesIgAnephropathy in Adults Treatments Standard NDT 2023lavadoraabcNo ratings yet
- AKI in SepsisDocument45 pagesAKI in SepsisIkeBundaAdellulaNo ratings yet
- IgA Nephropathy Autoimmune Kidney DiseaseDocument11 pagesIgA Nephropathy Autoimmune Kidney Diseasesky.blueNo ratings yet
- IgA Nephropathy JournalDocument11 pagesIgA Nephropathy JournalerlisaNo ratings yet
- An Update On The Pathogenesis and Treatment of IgADocument12 pagesAn Update On The Pathogenesis and Treatment of IgAYulius DonyNo ratings yet
- How Is IgA Nephropathy TreatedDocument2 pagesHow Is IgA Nephropathy TreatedRees SkaranNo ratings yet
- PPIs and Kidney DiseaseDocument6 pagesPPIs and Kidney DiseaseSonia jolandaNo ratings yet
- Rare NephroDocument16 pagesRare NephroMaria José GFNo ratings yet
- Toxicology PDFDocument8 pagesToxicology PDFsalwaNo ratings yet
- Iga Nephropathy With Pregnancy: Mr. Nasser B Mohamed, M.B. B.CH, MrcogDocument7 pagesIga Nephropathy With Pregnancy: Mr. Nasser B Mohamed, M.B. B.CH, Mrcogskolar01No ratings yet
- IJG 0b013e3182595075Document5 pagesIJG 0b013e3182595075EmirgibraltarNo ratings yet
- NefIgArd TrialDocument12 pagesNefIgArd Trialfarah mujtabaNo ratings yet
- Allopurinol-Induced Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) Syndrome Complicated by Acute Renal Failure - Cochrane LibraryDocument3 pagesAllopurinol-Induced Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) Syndrome Complicated by Acute Renal Failure - Cochrane LibraryJoc HerreraNo ratings yet
- An Open Label Study Evaluating The Safety and Efficacy of Budesonide in Patients With Iga Nephropathy at High Risk of ProgressionDocument11 pagesAn Open Label Study Evaluating The Safety and Efficacy of Budesonide in Patients With Iga Nephropathy at High Risk of ProgressionMukesh DassaniNo ratings yet
- Amelioration of Early Markers of Diabetic Nephropathy by Linagliptin in Fructose-Streptozotocin-Induced Type 2 Diabetic RatsDocument14 pagesAmelioration of Early Markers of Diabetic Nephropathy by Linagliptin in Fructose-Streptozotocin-Induced Type 2 Diabetic Ratsmohammed fayedNo ratings yet
- Immunoglobulina Nephropathyand Immunoglobulinavasculitis: Oana Nicoara,, Katherine TwombleyDocument10 pagesImmunoglobulina Nephropathyand Immunoglobulinavasculitis: Oana Nicoara,, Katherine TwombleyJéssica MorenoNo ratings yet
- Histologia, Conceitos Básicos Dos Tecidos - GitiranaDocument13 pagesHistologia, Conceitos Básicos Dos Tecidos - GitiranaJhonnatam EliasNo ratings yet
- Nsaid and KidneyDocument9 pagesNsaid and KidneyAndi Ade NurqalbiNo ratings yet
- Biomedicines: Advances in The Pharmacological Management of Diabetic Nephropathy: A 2022 International UpdateDocument15 pagesBiomedicines: Advances in The Pharmacological Management of Diabetic Nephropathy: A 2022 International Updatehenry leonardo gaona pinedaNo ratings yet
- Fimmu 13 921864Document17 pagesFimmu 13 921864Esteban TapiaNo ratings yet
- DN 8TH Sem Project FinalDocument30 pagesDN 8TH Sem Project FinalBhoj RajNo ratings yet
- SSNS CompressedDocument78 pagesSSNS CompressedVarun KotaNo ratings yet
- Iga Nephropathy (Berger'S Disease) : PathophysiologyDocument3 pagesIga Nephropathy (Berger'S Disease) : PathophysiologyEzyan SyaminNo ratings yet
- Sta Final PPT Team A Done (1) - 1Document26 pagesSta Final PPT Team A Done (1) - 1Sumi FaNo ratings yet
- Chap128 Terapi GNA PDFDocument4 pagesChap128 Terapi GNA PDFnovaNo ratings yet
- 1 s2.0 S2589537021005216 MainDocument13 pages1 s2.0 S2589537021005216 MainElena CuibanNo ratings yet
- Second Protein Causing Hereditary NTGDocument5 pagesSecond Protein Causing Hereditary NTGTalha Iftekhar KhanNo ratings yet
- Jurnal Comentary DirectDocument3 pagesJurnal Comentary DirectNurul AmaliaNo ratings yet
- SN CR 1Document3 pagesSN CR 1AmeldaNo ratings yet
- Review Article: Saudi Journal of Kidney Diseases and TransplantationDocument10 pagesReview Article: Saudi Journal of Kidney Diseases and TransplantationPedia PisoNo ratings yet
- TNF ALPHA in Neuropatia Diabetica Articol 2017Document6 pagesTNF ALPHA in Neuropatia Diabetica Articol 2017Pilat BogdanNo ratings yet
- 10 Primary Glumerulopathies III - GKDocument2 pages10 Primary Glumerulopathies III - GKGerarld Immanuel KairupanNo ratings yet
- Claudio Ronco, MD, Dinna Cruz, MD, and Brian W. Noland, PHDDocument8 pagesClaudio Ronco, MD, Dinna Cruz, MD, and Brian W. Noland, PHDDpto. ReferenciaNo ratings yet
- Nsaids and Kidney: P Ejaz, K Bhojani, VR JoshiDocument9 pagesNsaids and Kidney: P Ejaz, K Bhojani, VR JoshiSatrio AjieNo ratings yet
- Approach ConsiderationsDocument12 pagesApproach ConsiderationsTyna Mew-mewNo ratings yet
- Part 9. Approach To Chronic Kidney Disease Using These GuidelinesDocument8 pagesPart 9. Approach To Chronic Kidney Disease Using These GuidelinesSudjarwo AntonNo ratings yet
- Biopsy Proven Acute Interstitia Nephritis Secondary To Non-Steroidal Anti-Inflammatory Drugs Abuse in A Sixty Two Year Old ManDocument5 pagesBiopsy Proven Acute Interstitia Nephritis Secondary To Non-Steroidal Anti-Inflammatory Drugs Abuse in A Sixty Two Year Old ManIJAR JOURNALNo ratings yet
- New & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009Document42 pagesNew & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009farmasi_hmNo ratings yet
- Conservative Management of Chronic Renal Failure: Contemporary IssueDocument6 pagesConservative Management of Chronic Renal Failure: Contemporary IssueInes TerraheNo ratings yet
- Elevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A NephropathyDocument5 pagesElevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A Nephropathyagustinaw1981No ratings yet
- Acute Kidney Injury: KDIGO 2012 Clinical Practice GuidelineDocument40 pagesAcute Kidney Injury: KDIGO 2012 Clinical Practice GuidelineAbedDabajaNo ratings yet
- Research Study JournalDocument27 pagesResearch Study JournalHyacinth A RotaNo ratings yet
- Zomen in CKDDocument12 pagesZomen in CKDClaudiu BalabanNo ratings yet
- Article 1576845020 PDFDocument5 pagesArticle 1576845020 PDFFatima Habib JajjaNo ratings yet
- Allopurinol-Induced Drug Reactions With Eosinophilia and Systemic Symptoms Syndrome With Interstitial NephritisDocument12 pagesAllopurinol-Induced Drug Reactions With Eosinophilia and Systemic Symptoms Syndrome With Interstitial NephritisJoc HerreraNo ratings yet
- Management of IgA Vasculitis Nephritis (Henoch-Schonlein PurupuraDocument15 pagesManagement of IgA Vasculitis Nephritis (Henoch-Schonlein PurupuraGaling Chandika PutraNo ratings yet
- SRNS 2021Document44 pagesSRNS 2021Varun KotaNo ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- RecommendationsforSustainableInvestmentProducts AMAS SSFDocument26 pagesRecommendationsforSustainableInvestmentProducts AMAS SSFpetesqueeler7052No ratings yet
- Physics Exam QuestionsDocument8 pagesPhysics Exam Questionspetesqueeler7052No ratings yet
- DAC V3 Readme - BDocument61 pagesDAC V3 Readme - Bpetesqueeler7052No ratings yet
- Hex MapperDocument12 pagesHex Mapperpetesqueeler7052No ratings yet
- Differentiate Between: Defibrillation CardioversionDocument3 pagesDifferentiate Between: Defibrillation CardioversionStephy SojanNo ratings yet
- Course Exercise - PALS Precourse Self-Assessment and Precourse WorkDocument3 pagesCourse Exercise - PALS Precourse Self-Assessment and Precourse WorkPRICINo ratings yet
- Systematic ReviewDocument10 pagesSystematic ReviewLeeyaa CullenNo ratings yet
- Dr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiDocument124 pagesDr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiazizhaNo ratings yet
- Transesophageal EchocardiogramDocument3 pagesTransesophageal EchocardiogramsiddharthaNo ratings yet
- Heart Failure Treatment Algorithm: Diagnosis and ClassificationDocument7 pagesHeart Failure Treatment Algorithm: Diagnosis and ClassificationLorreine Elisa FaruqNo ratings yet
- Board 14 Desember 2014 Kumpulan FinalDocument73 pagesBoard 14 Desember 2014 Kumpulan FinalAnonymous XHguqDfWR0% (1)
- American Journal of Emergency Medicine: J. Rabjohns, T. Quan, K. Boniface, A. PourmandDocument5 pagesAmerican Journal of Emergency Medicine: J. Rabjohns, T. Quan, K. Boniface, A. Pourmandmaria Luisa VillaseñorNo ratings yet
- EcgDocument86 pagesEcgHidayatul ゆきNo ratings yet
- Diagnosis of Transposition of The Great ArteriesDocument7 pagesDiagnosis of Transposition of The Great ArteriesherryNo ratings yet
- Internal Medicine Lecture 6 Cardiomyopathies and MyocarditidesDocument98 pagesInternal Medicine Lecture 6 Cardiomyopathies and MyocarditidesDaily MedicineNo ratings yet
- Kidney Injury: AcuteDocument14 pagesKidney Injury: AcutealfredoibcNo ratings yet
- IntroductionDocument4 pagesIntroductionCristina L. JaysonNo ratings yet
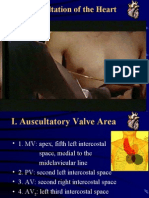
- Auscultation of HeartDocument92 pagesAuscultation of Heartsanjivdas100% (1)
- Nstemi Referenced Dosing GuideDocument3 pagesNstemi Referenced Dosing Guideriasali100% (1)
- IgA NephrophathyDocument4 pagesIgA NephrophathyyousifNo ratings yet
- Esc Beta Blocker Expert ConsensusDocument1 pageEsc Beta Blocker Expert ConsensusAkhmad HidayatNo ratings yet
- SDJ 2023 Last AnnDocument11 pagesSDJ 2023 Last AnnAstutiningrum Puspa DamayantiNo ratings yet
- Organizing Committee: AdvisorDocument22 pagesOrganizing Committee: AdvisorAnggit PudjiastutiNo ratings yet
- Schedule D: List of Life Saveing or Life Sustaining Medical DevicesDocument5 pagesSchedule D: List of Life Saveing or Life Sustaining Medical DevicesAasma RehmanNo ratings yet
- Topic: Cardiac Arrest Megacode: MD Khairulamin AS Nursing Lecturer PAPRSB Institute of Health Sciences UBDDocument38 pagesTopic: Cardiac Arrest Megacode: MD Khairulamin AS Nursing Lecturer PAPRSB Institute of Health Sciences UBDulipah100% (2)
- Echocardiography in CADDocument68 pagesEchocardiography in CADbalas4u89No ratings yet
- Rol HPNDocument5 pagesRol HPNOamaga NajlaNo ratings yet
- CV DrugsDocument6 pagesCV DrugssaharamichaelNo ratings yet
- (First Author) 2013 American Journal of Kidney Diseases 1Document5 pages(First Author) 2013 American Journal of Kidney Diseases 1Mahesh T MadhavanNo ratings yet