You might also like
- Nsarovo PDFDocument8 pagesNsarovo PDFMostafa FayadNo ratings yet
- Occlusion For StabilityDocument8 pagesOcclusion For StabilitydrsmritiNo ratings yet
- Occlusal Principles for Implants: An OverviewDocument5 pagesOcclusal Principles for Implants: An OverviewKrupali JainNo ratings yet
- Concepts of Arrangement of Artifical Teeth, SelectiveDocument7 pagesConcepts of Arrangement of Artifical Teeth, SelectiveAmar BhochhibhoyaNo ratings yet
- Occlusal philosophies in full-mouth rehabilitation literature reviewDocument4 pagesOcclusal philosophies in full-mouth rehabilitation literature reviewaggrolNo ratings yet
- Concepts of Arrangement of Artifical Teeth, Selective Grinding and Balanced Occlusion in Complete Denture ProsthodonticsDocument7 pagesConcepts of Arrangement of Artifical Teeth, Selective Grinding and Balanced Occlusion in Complete Denture ProsthodonticsHujarNo ratings yet
- ISSN: 0975-833X: Case StudyDocument3 pagesISSN: 0975-833X: Case StudyDeya rahmadhanyNo ratings yet
- Occlusal Concepts in Complete Denture Prosthodontics: A Literature ReviewDocument5 pagesOcclusal Concepts in Complete Denture Prosthodontics: A Literature ReviewSahana RangarajanNo ratings yet
- EBSCO FullText 2023 11 07Document8 pagesEBSCO FullText 2023 11 07Gianna LirianoNo ratings yet
- The Importance of OcclusionDocument7 pagesThe Importance of OcclusionZahra ZaNo ratings yet
- Occlusal Splint Therapy-Review Article: March 2013Document12 pagesOcclusal Splint Therapy-Review Article: March 2013Riya KvNo ratings yet
- Occlusion and Occlusal Considerations in Implantology: I J D ADocument6 pagesOcclusion and Occlusal Considerations in Implantology: I J D AJASPREETKAUR0410No ratings yet
- Review Article: Concepts of Complete Denture Occlusion: An Imperative Review of LiteratureDocument1 pageReview Article: Concepts of Complete Denture Occlusion: An Imperative Review of LiteratureSahana RangarajanNo ratings yet
- Oclusion OralDocument8 pagesOclusion OralzayraNo ratings yet
- TRP Greene StrubOcclusioDocument9 pagesTRP Greene StrubOcclusiodea swastikaNo ratings yet
- The Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewDocument10 pagesThe Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewFrancisca Dinamarca LamaNo ratings yet
- Occlusal SplintDocument12 pagesOcclusal SplintAmalia SalsabilaNo ratings yet
- Occlusal Designs On Masticatory Ability and Patient Satisfaction With Complete Denture - A Systematic ReviewDocument8 pagesOcclusal Designs On Masticatory Ability and Patient Satisfaction With Complete Denture - A Systematic ReviewMi Bazarcito PalmaritoNo ratings yet
- Occlusion: 2. Occlusal Splints, Analysis and Adjustment: Dental Update November 2003Document7 pagesOcclusion: 2. Occlusal Splints, Analysis and Adjustment: Dental Update November 2003Mostafa HassanNo ratings yet
- 1972 Occlusion in Removable Partial Prosthodontics - HendersonDocument9 pages1972 Occlusion in Removable Partial Prosthodontics - HendersontovarichNo ratings yet
- Dental Occlusion A Newly Proposed TetrahDocument10 pagesDental Occlusion A Newly Proposed TetrahIlinca LupuNo ratings yet
- Waxing Techniques To Develop Proper Occlusal Morphology in Different Occlusal SchemesDocument6 pagesWaxing Techniques To Develop Proper Occlusal Morphology in Different Occlusal SchemesMihaela VasiliuNo ratings yet
- Occlusal Concepts in Full Mouth Rehabilitation: An OverviewDocument8 pagesOcclusal Concepts in Full Mouth Rehabilitation: An OverviewShanna MitchellNo ratings yet
- Dental Occlusion A Critical Reflectionon Past Present and FutureDocument8 pagesDental Occlusion A Critical Reflectionon Past Present and FutureplsssssNo ratings yet
- Dental Occlusion: Proposal For A Classification To Guide Occlusal Analysis and Optimize Research ProtocolsDocument10 pagesDental Occlusion: Proposal For A Classification To Guide Occlusal Analysis and Optimize Research ProtocolsAARON DIAZ RONQUILLONo ratings yet
- 2020 Khushboo MishraDocument8 pages2020 Khushboo Mishra謎超人No ratings yet
- 1-5 Occlusion in Removable Partial ProsthodonticsDocument5 pages1-5 Occlusion in Removable Partial ProsthodonticsIlse100% (1)
- Occlusion: Orthodontics and Occlusion: British Dental Journal December 2001Document10 pagesOcclusion: Orthodontics and Occlusion: British Dental Journal December 2001Naeem MoollaNo ratings yet
- 1 s2.0 S002239131360030X MainDocument6 pages1 s2.0 S002239131360030X MainAmar Bhochhibhoya100% (1)
- Dental Occlusion Proposal For A ClassifiDocument10 pagesDental Occlusion Proposal For A ClassifiDoctor JackNo ratings yet
- Optimal Vs Ideal OcclusionDocument6 pagesOptimal Vs Ideal OcclusionshraddhaNo ratings yet
- Article 32Document9 pagesArticle 32Lenny GrauNo ratings yet
- Review Article: Occlusal Schemes For Complete Dentures - A Review ArticleDocument6 pagesReview Article: Occlusal Schemes For Complete Dentures - A Review ArticleoktikikiNo ratings yet
- An Evidence-Based Evaluation of The Concept of Centric Relation in The 21st CenturyDocument6 pagesAn Evidence-Based Evaluation of The Concept of Centric Relation in The 21st Centuryilich sevilla100% (1)
- JIndianProsthodontSoc184321-4265876 115058Document8 pagesJIndianProsthodontSoc184321-4265876 115058Dr FarhatNo ratings yet
- Complete Denture Occlusion PDFDocument25 pagesComplete Denture Occlusion PDFÄpriolia SuNo ratings yet
- Occlusion in RPDDocument5 pagesOcclusion in RPDDhananjay GandageNo ratings yet
- Occlusion in Implant DentistryDocument9 pagesOcclusion in Implant DentistrydrsmritiNo ratings yet
- Prosthodontic Care For Patients With Cleft PalateDocument7 pagesProsthodontic Care For Patients With Cleft PalateValery V JaureguiNo ratings yet
- Diagnosis and Management of Occlusal Wear: A Case ReportDocument7 pagesDiagnosis and Management of Occlusal Wear: A Case ReportAya KassemNo ratings yet
- Aos Occlusal OverviewDocument8 pagesAos Occlusal OverviewnadiaNo ratings yet
- Occlusion Orthodontics and OcclusionDocument10 pagesOcclusion Orthodontics and OcclusionSaherishNo ratings yet
- Coronoplasty 2Document4 pagesCoronoplasty 2Befalia Aisarahmadani100% (1)
- Art 2Document6 pagesArt 2Joyce Stefania Posada MauricioNo ratings yet
- 2013 Sagar J AbichandaniDocument8 pages2013 Sagar J Abichandani謎超人No ratings yet
- Occlusal Forms and Philosophies in Full Mouth Rehabilitation: A Literature ReviewDocument5 pagesOcclusal Forms and Philosophies in Full Mouth Rehabilitation: A Literature ReviewSkAliHassanNo ratings yet
- Fox 1983Document9 pagesFox 1983avi pahwaNo ratings yet
- J of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsDocument6 pagesJ of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsManuel CastilloNo ratings yet
- J of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsDocument6 pagesJ of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsVasu SinghNo ratings yet
- Bone Anchored Maxillary Protraction 2012 American Journal of Orthodontics and Dentofacial OrthopedicsDocument2 pagesBone Anchored Maxillary Protraction 2012 American Journal of Orthodontics and Dentofacial OrthopedicsjosemtzzNo ratings yet
- Occlusion For Implant Suppported CD PDFDocument4 pagesOcclusion For Implant Suppported CD PDFFabián SajamaNo ratings yet
- Centric Relation Critically Revisited - What Are The Clinical ImplicationDocument6 pagesCentric Relation Critically Revisited - What Are The Clinical ImplicationAlejandro RuizNo ratings yet
- N Zone Article PDFDocument5 pagesN Zone Article PDFBintilsultan AL-JubooryNo ratings yet
- JIntOralHealth85639-2083732 054717 PDFDocument7 pagesJIntOralHealth85639-2083732 054717 PDFVivek ShankarNo ratings yet
- JIntOralHealth85639-2083732 054717 PDFDocument7 pagesJIntOralHealth85639-2083732 054717 PDFVivek ShankarNo ratings yet
- The Monoplane Occlusion For Complete Dentures: T H e SP Herical TheoryDocument7 pagesThe Monoplane Occlusion For Complete Dentures: T H e SP Herical TheorySahana RangarajanNo ratings yet
- Occlusion As Reked To Co Prosthodontics Refrtow E: Complete DenturesDocument11 pagesOcclusion As Reked To Co Prosthodontics Refrtow E: Complete DenturesKrupali JainNo ratings yet
- Space Regainers in Pediatric Dentistry: January 2015Document6 pagesSpace Regainers in Pediatric Dentistry: January 2015Fajar Kusuma Dwi KurniawanNo ratings yet
- FMR OcclusionDocument10 pagesFMR OcclusionSkAliHassanNo ratings yet
- MDS Prosthodontics New CurriculumDocument54 pagesMDS Prosthodontics New CurriculumPriyanka GandhiNo ratings yet
- Lasers in Prosthodontics - A Review: Prosthetic and Implant DentistryDocument7 pagesLasers in Prosthodontics - A Review: Prosthetic and Implant DentistryPriyanka GandhiNo ratings yet
- Accuracy and Reliability of Methods To Measure Marginal Adaptation of Crowns and FDPS: A Literature ReviewDocument10 pagesAccuracy and Reliability of Methods To Measure Marginal Adaptation of Crowns and FDPS: A Literature ReviewPriyanka GandhiNo ratings yet
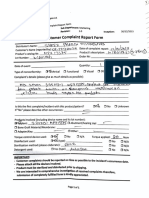
- Dr. Priyanka. Implant Complaint FormDocument2 pagesDr. Priyanka. Implant Complaint FormPriyanka GandhiNo ratings yet
- Smile Design: Nicholas C. Davis, DDS, MAGDDocument20 pagesSmile Design: Nicholas C. Davis, DDS, MAGDPriyanka GandhiNo ratings yet
- EJMCM - Volume 7 - Issue 2 - Pages 6784-6789Document6 pagesEJMCM - Volume 7 - Issue 2 - Pages 6784-6789Priyanka GandhiNo ratings yet
- Applied Basic SciencesDocument2 pagesApplied Basic SciencesPriyanka GandhiNo ratings yet
- Surveying: British Dental Journal Official Journal of The British Dental Association: BDJ Online December 2000Document12 pagesSurveying: British Dental Journal Official Journal of The British Dental Association: BDJ Online December 2000andreas kevinNo ratings yet
- Uses, Accuracy and Limitations of Semiadjustable Articulators in Dentistry: A Systematic ReviewDocument15 pagesUses, Accuracy and Limitations of Semiadjustable Articulators in Dentistry: A Systematic ReviewPriyanka GandhiNo ratings yet
- Surveying: British Dental Journal Official Journal of The British Dental Association: BDJ Online December 2000Document12 pagesSurveying: British Dental Journal Official Journal of The British Dental Association: BDJ Online December 2000andreas kevinNo ratings yet
- Failures in Fixed Partial Dentures: Dr. Rohit FernandezDocument89 pagesFailures in Fixed Partial Dentures: Dr. Rohit FernandezPriyanka GandhiNo ratings yet
- Dental Articulator & Face-Bow: ProsthodonticsDocument12 pagesDental Articulator & Face-Bow: ProsthodonticsPriyanka GandhiNo ratings yet
- M.D.S. Final Year Exams for 8 Dental BranchesDocument6 pagesM.D.S. Final Year Exams for 8 Dental BranchesPriyanka GandhiNo ratings yet
- GCC Specialist RecruitmentDocument5 pagesGCC Specialist RecruitmentPriyanka GandhiNo ratings yet
- Tax Invoice for Dental SuppliesDocument2 pagesTax Invoice for Dental SuppliesPriyanka GandhiNo ratings yet
- JCDP 19 624Document4 pagesJCDP 19 624Priyanka GandhiNo ratings yet
- MDS Pract DtMay2021Document1 pageMDS Pract DtMay2021Priyanka GandhiNo ratings yet
- MDS CC 1Document1 pageMDS CC 1Priyanka GandhiNo ratings yet
- Web Message November 2021 Examination Final Year Mds Degree CourseDocument1 pageWeb Message November 2021 Examination Final Year Mds Degree CoursePriyanka GandhiNo ratings yet
- Occlusal appliance therapy for TMD patientsDocument7 pagesOcclusal appliance therapy for TMD patientsPriyanka GandhiNo ratings yet
- W Eb Message March 202 2 Examination First Year Mds Degree CourseDocument1 pageW Eb Message March 202 2 Examination First Year Mds Degree CoursePriyanka GandhiNo ratings yet
- SC and Rett 1978Document3 pagesSC and Rett 1978Priyanka GandhiNo ratings yet
- Reorganising Occlusion PrinciplesDocument4 pagesReorganising Occlusion PrinciplesPriyanka GandhiNo ratings yet
- c21 Art2 Esthetic AnalysisDocument8 pagesc21 Art2 Esthetic AnalysisPriyanka GandhiNo ratings yet
- Lesson TemplateDocument6 pagesLesson TemplateAnonymous 9p23ZapzNo ratings yet
- Head and NeckDocument11 pagesHead and NeckdrsamnNo ratings yet
- Teaching Methods Ballet 1 ClassDocument10 pagesTeaching Methods Ballet 1 ClassNicoleMakenaBrowneNo ratings yet
- Integumentary System Terminology WorksheetDocument2 pagesIntegumentary System Terminology WorksheetfernandaNo ratings yet
- Reading Homework June 19Document2 pagesReading Homework June 19Anna Jean FernandezNo ratings yet
- Pages 183 Physiological Psychology MCQ 1Document34 pagesPages 183 Physiological Psychology MCQ 1AdsNo ratings yet
- Object Localization TechniquesDocument19 pagesObject Localization TechniquesAbdullah El-Zaabout100% (3)
- Trigeminal NerveDocument131 pagesTrigeminal NerveLavanya KalapalaNo ratings yet
- Master Perfect Handstand Body MechanicsDocument9 pagesMaster Perfect Handstand Body MechanicsAlejandro Ket100% (1)
- New Ballard ScoreDocument39 pagesNew Ballard ScoreJAMES ROD MARINDUQUENo ratings yet
- Workout Program: Shortcut To SizeDocument12 pagesWorkout Program: Shortcut To SizeAhmed Hamza100% (2)
- Musculoskeletal History: Basic InfoDocument10 pagesMusculoskeletal History: Basic InfoTom MallinsonNo ratings yet
- Dr. Samahi's lecture on post-insertion denture problems and follow-up visitsDocument10 pagesDr. Samahi's lecture on post-insertion denture problems and follow-up visitsRahul MahajanNo ratings yet
- Anatomy index provides concise navigation of key structuresDocument7 pagesAnatomy index provides concise navigation of key structuresnour achkarNo ratings yet
- 1 The General Plan of PatientDocument7 pages1 The General Plan of PatientcorsairmdNo ratings yet
- Excretory System NotesDocument10 pagesExcretory System Noteswama ojha100% (1)
- Anatomy of Nervous TissueDocument54 pagesAnatomy of Nervous TissueNand PrakashNo ratings yet
- Box Jump From A Static Start: ExecutionDocument34 pagesBox Jump From A Static Start: Executioncoach_noeNo ratings yet
- Neuro 2 AnsDocument14 pagesNeuro 2 AnsSantiago AldayNo ratings yet
- Clubfoot Ponseti Management, 3rd Edition-1601890028Document32 pagesClubfoot Ponseti Management, 3rd Edition-1601890028Ankur MittalNo ratings yet
- Copy+of+AM+ +Frog+Dissection+ (Remote)Document21 pagesCopy+of+AM+ +Frog+Dissection+ (Remote)Khosraw HalimiNo ratings yet
- Siop Model Weightlifting Lesson Plan PowerpointDocument23 pagesSiop Model Weightlifting Lesson Plan Powerpointapi-652792108No ratings yet
- Anatomy Lower LimbDocument4 pagesAnatomy Lower Limbch yaqoobNo ratings yet
- Local Flap Reconstruction of Large Scalp DefectsDocument5 pagesLocal Flap Reconstruction of Large Scalp DefectsPalwasha MalikNo ratings yet
- Circulation in AnnelidaDocument2 pagesCirculation in AnnelidaNarasimha MurthyNo ratings yet
- Stevens&Lowes Human Histology 4 EDocument452 pagesStevens&Lowes Human Histology 4 Eusuario desconocido100% (1)
- Clinical Examination of The Ulnar-Sided Painful Wrist: Marc Garcia-EliasDocument20 pagesClinical Examination of The Ulnar-Sided Painful Wrist: Marc Garcia-EliasMadhusudhan Acharya100% (1)
- Heart Dissection Lab Report Guide2Document7 pagesHeart Dissection Lab Report Guide2Dylan FernandezNo ratings yet
- Chronology of Human Dentition & Tooth Numbering SystemDocument54 pagesChronology of Human Dentition & Tooth Numbering Systemdr parveen bathla100% (4)
- Assessment of Nose Mouth Pharynx Unit 5 1Document36 pagesAssessment of Nose Mouth Pharynx Unit 5 1MUHAMMAD SALMANNo ratings yet