You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lab 7 RC Time ConstantDocument8 pagesLab 7 RC Time ConstantMalith Madushan100% (1)
- Transformer and Inductor Design Handbook (PDFDrive)Document669 pagesTransformer and Inductor Design Handbook (PDFDrive)nirwana84No ratings yet
- ABB - Protectii Fotovoltaice, Protectii - FotovoltaiceDocument20 pagesABB - Protectii Fotovoltaice, Protectii - FotovoltaiceIeremeiov Vladimir100% (1)
- Nissan RE0F09A: Preliminary InformationDocument9 pagesNissan RE0F09A: Preliminary Informationmech5455100% (3)
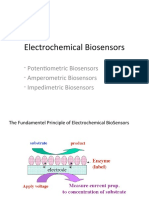
- Electrochemical Biosensors: - Potentiometric Biosensors - Amperometric Biosensors - Impedimetric BiosensorsDocument18 pagesElectrochemical Biosensors: - Potentiometric Biosensors - Amperometric Biosensors - Impedimetric BiosensorsutkuyavuzNo ratings yet
- 530ADD01 DS enDocument4 pages530ADD01 DS enHatem LaadhariNo ratings yet
- VHF FM Transceiver: Vertex Standard Co., Ltd. Vertex StandardDocument41 pagesVHF FM Transceiver: Vertex Standard Co., Ltd. Vertex Standardfazenda sao gabrielNo ratings yet
- Computer Hardware BookDocument336 pagesComputer Hardware BookbharathydglNo ratings yet
- Copeland AE1287 Demand CoolingDocument12 pagesCopeland AE1287 Demand CoolinggigiNo ratings yet
- Description: Family of Engine Control Modules - Calibratible / FlashDocument18 pagesDescription: Family of Engine Control Modules - Calibratible / FlashТетрис МанNo ratings yet
- Solis Manual RHI (3-6) K 5G ENX V1,5Document41 pagesSolis Manual RHI (3-6) K 5G ENX V1,5alessio “furiosbomba” lo medicoNo ratings yet
- Filter With S-Shaped Broadside Coupled Complementary Split Ring Resonators (BC-CSRR)Document8 pagesFilter With S-Shaped Broadside Coupled Complementary Split Ring Resonators (BC-CSRR)HAPURNo ratings yet
- Lecturer-21 Solid Dielectrics Used in Practice: High Voltage Engineering (Feee6402)Document6 pagesLecturer-21 Solid Dielectrics Used in Practice: High Voltage Engineering (Feee6402)r2patelNo ratings yet
- TLP521 4 PDFDocument3 pagesTLP521 4 PDFchafic WEISSNo ratings yet
- Cohr Dilas Compact Ac PKGDocument3 pagesCohr Dilas Compact Ac PKGPhan ÂnNo ratings yet
- ENG TechnicalDocument5 pagesENG TechnicalAnonymous hRePlgdOFrNo ratings yet
- Autonics CX Series - User ManualDocument87 pagesAutonics CX Series - User ManualEldglay da Silva DomingosNo ratings yet
- Wideband Dual-Circularly Polarized Antennas Using Aperture-Coupled Stacked Patches and Single-Section Hybrid CouplerDocument9 pagesWideband Dual-Circularly Polarized Antennas Using Aperture-Coupled Stacked Patches and Single-Section Hybrid Couplerdtvt2006No ratings yet
- Sunrom Catalog 21 Oct 2015Document16 pagesSunrom Catalog 21 Oct 2015Prabhat SagarNo ratings yet
- Magnetism and Matter All DerivationsDocument5 pagesMagnetism and Matter All DerivationsRonit VaskarNo ratings yet
- ICLP 2014 Conference Presentation Slides - FinalDocument22 pagesICLP 2014 Conference Presentation Slides - FinalsanibubaNo ratings yet
- Manual IC-A24 - A6Document41 pagesManual IC-A24 - A6jorge garciaNo ratings yet
- Chapter 22 Example of Maintenance 1Document7 pagesChapter 22 Example of Maintenance 1Ij OooNo ratings yet
- Detailed Lesson Plan Electropneumatics - No HeaderDocument5 pagesDetailed Lesson Plan Electropneumatics - No HeaderMarnie AstrologoNo ratings yet
- Simplex Installation Instructions Fire Fighter Phone System PDFDocument28 pagesSimplex Installation Instructions Fire Fighter Phone System PDFGuilherme QueróbiNo ratings yet
- EEE 111 ProjectsDocument8 pagesEEE 111 ProjectsAnik Saha Toni 1912619643No ratings yet
- Lighting and Small Power Works at New Ablution Room and New Male ToiletDocument10 pagesLighting and Small Power Works at New Ablution Room and New Male ToiletRoshan de SilvaNo ratings yet
- LG 42pc55 (ET)Document53 pagesLG 42pc55 (ET)Andy CoyneNo ratings yet
- Evaluation of Electrical PowerDocument16 pagesEvaluation of Electrical PowerMartins RichmondNo ratings yet
- Carrier ChillerDocument20 pagesCarrier ChillerElsayed KhamisNo ratings yet