You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lab Report 5Document7 pagesLab Report 5enieynazNo ratings yet
- Data Acquisition in MATLAB PDFDocument30 pagesData Acquisition in MATLAB PDFjaneprice100% (1)
- Work ImmersionDocument12 pagesWork ImmersionGerald TamondongNo ratings yet
- Practical 2: Investigating The Universe - Gravity: T, Depends On The Length of The String and The GDocument3 pagesPractical 2: Investigating The Universe - Gravity: T, Depends On The Length of The String and The GRegie Sacil EspiñaNo ratings yet
- Nist HB 162 MepsDocument170 pagesNist HB 162 MepsDavid GoldNo ratings yet
- Helping Kids Develop Conflict Resolution SkillsDocument3 pagesHelping Kids Develop Conflict Resolution SkillsDiya MariaNo ratings yet
- Bombs: Protecting People and PropertyDocument32 pagesBombs: Protecting People and PropertyantiqbabilonNo ratings yet
- Bolt Load Software: ANSI B16.5 Api 6A Api 17Sv Norsok L-005 SPO Compact Flanges Taperlok FlangesDocument2 pagesBolt Load Software: ANSI B16.5 Api 6A Api 17Sv Norsok L-005 SPO Compact Flanges Taperlok Flangesloveanbu24No ratings yet
- The Six Steps of The Writing ProcessDocument4 pagesThe Six Steps of The Writing ProcessBenjamín Fernando Rodriguez Santana67% (3)
- CPCCCM2007B Student Final Assessment Submission EvidenceDocument36 pagesCPCCCM2007B Student Final Assessment Submission Evidencemishal chNo ratings yet
- Unfpa YpeerDocument33 pagesUnfpa YpeerȜomar M Bani HaniNo ratings yet
- Discrete Math IntroductionDocument3 pagesDiscrete Math IntroductionNur FirdausNo ratings yet
- GIDA Profiling Tool Version 2 2018Document7 pagesGIDA Profiling Tool Version 2 2018NL R Q DO0% (1)
- Pessimist, Judge and RealistDocument1 pagePessimist, Judge and RealistProfessora Angela Faculdade Sant'AnaNo ratings yet
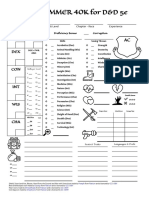
- WARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceDocument1 pageWARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceJacob CooperNo ratings yet
- CIA Exam:: Updated. Aligned. FocusedDocument7 pagesCIA Exam:: Updated. Aligned. FocusedveveNo ratings yet
- Mpspre TestnewDocument17 pagesMpspre TestnewMAE LOVE NABARRONo ratings yet
- Using Zend Framework 2Document506 pagesUsing Zend Framework 2JacquelineNahirSterembergNo ratings yet
- Chapter 8 (Compatibility Mode) Brand Equity MeasurementDocument15 pagesChapter 8 (Compatibility Mode) Brand Equity MeasurementMayank ToliaNo ratings yet
- Weld Joint Design and Weld SymbolDocument49 pagesWeld Joint Design and Weld SymbolArdser Avico100% (2)
- Intro To FemDocument83 pagesIntro To FemRavi MalikNo ratings yet
- Lesson Plan Bil 1Document2 pagesLesson Plan Bil 1Izatul Shima Abu SahidNo ratings yet
- (VigChr Supp 109) David T. Runia-Philo of Alexandria - An Annotated Bibliography 1997-2006 With Addenda For 1987-1996 (2011) PDFDocument519 pages(VigChr Supp 109) David T. Runia-Philo of Alexandria - An Annotated Bibliography 1997-2006 With Addenda For 1987-1996 (2011) PDFNovi Testamenti FiliusNo ratings yet
- Killzone Rules v3Document25 pagesKillzone Rules v3dracomaxisNo ratings yet
- Understanding Jyotish PrinciplesDocument5 pagesUnderstanding Jyotish PrinciplesSanjay Sinha100% (1)
- Lesson Plan in Practical Research 1Document4 pagesLesson Plan in Practical Research 1Dominica Recoy Pontica - DiololaNo ratings yet
- RESUMEDocument3 pagesRESUMESunny LamNo ratings yet
- MultiFlexETH UserManualDocument218 pagesMultiFlexETH UserManualrocketmenchNo ratings yet
- Rocket ReportDocument13 pagesRocket Reportapi-267418290No ratings yet
- Mec235 - Thermo FluidsDocument10 pagesMec235 - Thermo FluidsManish JainNo ratings yet