You might also like
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- Pulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveFrom EverandPulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveNo ratings yet
- Idsa 2018Document94 pagesIdsa 2018Gaby Galarza TaboadaNo ratings yet
- Esbl Producing eDocument45 pagesEsbl Producing eapi-205355237No ratings yet
- Necrotizing Facitis ReviewDocument16 pagesNecrotizing Facitis ReviewHadi Firmansyah SidiqNo ratings yet
- Patient Case - Vpa ToxicityDocument13 pagesPatient Case - Vpa Toxicityapi-611386981No ratings yet
- Prisma Health Adult Antimicrobial Guidebook 2021Document52 pagesPrisma Health Adult Antimicrobial Guidebook 2021JhNo ratings yet
- 2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDDocument30 pages2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDPeter Albeiro Falla CortesNo ratings yet
- Kee Gales CV October 2020Document8 pagesKee Gales CV October 2020api-523660034No ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- Antibiotic Stewardship PDFDocument11 pagesAntibiotic Stewardship PDFujangNo ratings yet
- The Who Treatment Protocol For MalariaDocument18 pagesThe Who Treatment Protocol For MalariatabletvodaNo ratings yet
- Cardiovascular Disease - by SlidesgoDocument95 pagesCardiovascular Disease - by SlidesgoDaniela OropezaNo ratings yet
- Pharmacology Antimycobacterial DrugsDocument9 pagesPharmacology Antimycobacterial Drugsroyce charlieNo ratings yet
- EDT007Document110 pagesEDT007mahchusNo ratings yet
- Cellulitis Oral Case PresDocument48 pagesCellulitis Oral Case PresLet BorlagdanNo ratings yet
- IDSA Guideline PDFDocument80 pagesIDSA Guideline PDFArifHidayatNo ratings yet
- Opat Ce Slides Final 2Document55 pagesOpat Ce Slides Final 2api-534233456No ratings yet
- Therapeutic Cooling Protocol for Perinatal AsphyxiaDocument31 pagesTherapeutic Cooling Protocol for Perinatal AsphyxiaNiraj GuptaNo ratings yet
- DVT Diagnostics ACCPDocument2 pagesDVT Diagnostics ACCPKholil ElsirajNo ratings yet
- OS217 LEC06 Rational Antibiotic UseDocument6 pagesOS217 LEC06 Rational Antibiotic Usegenerics54321No ratings yet
- Clabsi101 508Document53 pagesClabsi101 508Arjun KumarNo ratings yet
- Neutropenic Fever Empiric TherapyDocument5 pagesNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraNo ratings yet
- Vancomycin Auc With Answers 1Document64 pagesVancomycin Auc With Answers 1api-493355126No ratings yet
- Cestoda: Dr. Hendra (Tropmed) Parasitology Department Medical Faculty of UnpriDocument42 pagesCestoda: Dr. Hendra (Tropmed) Parasitology Department Medical Faculty of UnpriElvy ShaluNo ratings yet
- Quick Reference DMARDsDocument12 pagesQuick Reference DMARDsEman MohamedNo ratings yet
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- Bronchiectasis NishaDocument44 pagesBronchiectasis NishaKaarthigan RamaiahNo ratings yet
- Infective Endocarditis: Hariprasad KDocument28 pagesInfective Endocarditis: Hariprasad KHari Prasad K100% (1)
- Cell Wall and Membrane Disruption MechanismsDocument5 pagesCell Wall and Membrane Disruption MechanismsTrevorNo ratings yet
- Febril NetropeniDocument352 pagesFebril NetropeniDilessandro PieroNo ratings yet
- Arthroplasty JournalDocument3 pagesArthroplasty Journallina yohanes100% (1)
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- Anti-infective Agents Chapter OverviewDocument13 pagesAnti-infective Agents Chapter OverviewEricka AbellaNo ratings yet
- CV 2021Document5 pagesCV 2021api-611973258No ratings yet
- Salycilic AcidDocument46 pagesSalycilic AcidDarshit KalariyaNo ratings yet
- Fever with Chills and Rigors: A Case of MalariaDocument19 pagesFever with Chills and Rigors: A Case of MalariaREETHUNo ratings yet
- Anti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDocument41 pagesAnti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDr. Ashish JawarkarNo ratings yet
- Antimicrobial Therapy for Infectious DiseasesDocument212 pagesAntimicrobial Therapy for Infectious Diseasesaleen qawareetNo ratings yet
- Anaerobic InfectionsDocument36 pagesAnaerobic InfectionsPatriceNo ratings yet
- 4th Edition National Guidelines For Diagnosis and Treatment of MalariaDocument79 pages4th Edition National Guidelines For Diagnosis and Treatment of MalariaAbimbola PhillipsNo ratings yet
- Intracerebral Haemorrhage: Disease PrimersDocument18 pagesIntracerebral Haemorrhage: Disease PrimersMarlon VillanuevaNo ratings yet
- The Doctors in ICU Need To Know The Basics Of.2Document9 pagesThe Doctors in ICU Need To Know The Basics Of.2Santiago Chávez100% (1)
- SDPSC Icu Sedation Guidelines of Care Toolkit December 2009Document44 pagesSDPSC Icu Sedation Guidelines of Care Toolkit December 2009yonoNo ratings yet
- Management of GNR BacteremiaDocument18 pagesManagement of GNR Bacteremiaapi-602288180No ratings yet
- Hospital Pharmacy Policy ManualDocument3 pagesHospital Pharmacy Policy ManualdmuscleNo ratings yet
- Aminoglycoside AntibioticsDocument56 pagesAminoglycoside AntibioticsMaharani IndriatyNo ratings yet
- Carbapenamses in Antibiotic ResistanceDocument53 pagesCarbapenamses in Antibiotic Resistancetummalapalli venkateswara raoNo ratings yet
- Systemic Fungal InfectionDocument43 pagesSystemic Fungal InfectionDarian DavinNo ratings yet
- Anne Gershon (Editor), Peter Hotez (Editor), Samuel Katz (Editor) - Krugman's Infectious Diseases of Children-Mosby, in PDFDocument2,854 pagesAnne Gershon (Editor), Peter Hotez (Editor), Samuel Katz (Editor) - Krugman's Infectious Diseases of Children-Mosby, in PDFyudhoNo ratings yet
- MycobacteriumDocument11 pagesMycobacteriumskNo ratings yet
- Rational Antibiotic Usage and Antibiotic Policy - Dr. FirmansyahDocument76 pagesRational Antibiotic Usage and Antibiotic Policy - Dr. Firmansyahjay neefNo ratings yet
- Anaerobic Bacterias GuideDocument11 pagesAnaerobic Bacterias GuideSanjay ShresthaNo ratings yet
- DR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDocument27 pagesDR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDhiraj PantNo ratings yet
- Bcps - AcsDocument63 pagesBcps - Acsapi-506607906No ratings yet
- Surgical Prophylaxis and Antibiotic Selection Guide /TITLEDocument37 pagesSurgical Prophylaxis and Antibiotic Selection Guide /TITLEAbanoub Nabil100% (1)
- Aminoglycoside Dosing GuidelinesDocument3 pagesAminoglycoside Dosing GuidelinesaeromintNo ratings yet
- Chapter 12 Drugs, Microbes, The Elements of Chemotherapy: Building Your KnowledgeDocument12 pagesChapter 12 Drugs, Microbes, The Elements of Chemotherapy: Building Your Knowledgemalenya1100% (1)
- PyomeningitisDocument54 pagesPyomeningitisRiya BagdiNo ratings yet
- Hemolytic Uremic Syndrome - Case Report: MædicaDocument3 pagesHemolytic Uremic Syndrome - Case Report: MædicaEstellaNo ratings yet
- Primary Adrenal Insufficiency HandoutDocument2 pagesPrimary Adrenal Insufficiency Handoutapi-614156568No ratings yet
- Purdy Teaching Experience Log 2021-2022Document4 pagesPurdy Teaching Experience Log 2021-2022api-614156568No ratings yet
- Purdy Grand Rounds Capa Final DraftDocument30 pagesPurdy Grand Rounds Capa Final Draftapi-614156568No ratings yet
- Bcps LectureDocument60 pagesBcps Lectureapi-614156568No ratings yet
- Encephalopathy and Cirrhosis Family Medicine PresentationDocument23 pagesEncephalopathy and Cirrhosis Family Medicine Presentationapi-614156568No ratings yet
- Biostatistics Ce PresentationDocument62 pagesBiostatistics Ce Presentationapi-614156568No ratings yet
- Purdy Andrew Curriculum VitaeDocument8 pagesPurdy Andrew Curriculum Vitaeapi-614156568No ratings yet
- Vivas in Surgical Pathology For DM 1: What Is A Neoplasm? Define Neoplasia?Document11 pagesVivas in Surgical Pathology For DM 1: What Is A Neoplasm? Define Neoplasia?Giovanni HenryNo ratings yet
- Eukaryotic Gene RegulationDocument79 pagesEukaryotic Gene RegulationLucky SatapathyNo ratings yet
- Bee Products in Dermatology and Skin Care: ReviewDocument17 pagesBee Products in Dermatology and Skin Care: ReviewwizuraihakimroyNo ratings yet
- Genomics-Lectures 1 To 8 - 2023 PDFDocument110 pagesGenomics-Lectures 1 To 8 - 2023 PDFAhire Ganesh Ravindra bs20b004No ratings yet
- Appendix 2 Colposcopy ManagementDocument2 pagesAppendix 2 Colposcopy ManagementFA KhanNo ratings yet
- Biochemistry For Medical Laboratory Science Course Outline 2018Document4 pagesBiochemistry For Medical Laboratory Science Course Outline 2018Vincent Cuyuca100% (1)
- Introduction to Human Body SystemsDocument7 pagesIntroduction to Human Body SystemsPriya YadavNo ratings yet
- EUA Healgen Rapid Ifu PDFDocument4 pagesEUA Healgen Rapid Ifu PDFMuhammad Khairul HakimiNo ratings yet
- Dr. Alfadel Alshaibani - Hematology Board ReviewDocument258 pagesDr. Alfadel Alshaibani - Hematology Board ReviewHanadi UmhanayNo ratings yet
- Technical Glitches in Micropropagation: Saurabh Bhatia, Kiran SharmaDocument12 pagesTechnical Glitches in Micropropagation: Saurabh Bhatia, Kiran Sharma38 Sourav BhowmikNo ratings yet
- The Barbastro ReportDocument8 pagesThe Barbastro ReportCraig StoneNo ratings yet
- Sensory PolyneuropathiesDocument26 pagesSensory PolyneuropathiesAnderson TravassosNo ratings yet
- Bacterial Identification in Endodontic InfectionsDocument6 pagesBacterial Identification in Endodontic InfectionsFajri NurNo ratings yet
- Transport in Humans: Test Yourself 8.1 (Page 140)Document3 pagesTransport in Humans: Test Yourself 8.1 (Page 140)lee100% (3)
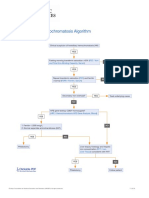
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- Phagocytosis Block 5Document25 pagesPhagocytosis Block 5Mark Johnuel DuavisNo ratings yet
- 3 Population GeneticsDocument95 pages3 Population GeneticsYuhua SunNo ratings yet
- Infection Control in Dental RadiologyDocument41 pagesInfection Control in Dental RadiologyDrShweta Saini0% (1)
- Early March, Meiosis - Mitosis Study Guide (3.3)Document9 pagesEarly March, Meiosis - Mitosis Study Guide (3.3)ChanelleNo ratings yet
- Core CH 27 Molecular GeneticsDocument6 pagesCore CH 27 Molecular GeneticsTSZ YAN CHEUNGNo ratings yet
- Recent Advances in Anaesthesia and Intensive CareDocument323 pagesRecent Advances in Anaesthesia and Intensive CaresurasuarezlopezNo ratings yet
- Chapter 20 Solutions Molecular Biology of The CellDocument15 pagesChapter 20 Solutions Molecular Biology of The CellAkshey BadrinarayanNo ratings yet
- Major functions of adrenergic and cholinergic receptorsDocument77 pagesMajor functions of adrenergic and cholinergic receptorsBetsy Brown Byersmith100% (1)
- Intramyocardial Inflammation After COVID-19 VaccineDocument13 pagesIntramyocardial Inflammation After COVID-19 VaccineJim HoftNo ratings yet
- 台大 檢驗醫學部檢驗項目參考值 (A3) PDFDocument1 page台大 檢驗醫學部檢驗項目參考值 (A3) PDFalex wuNo ratings yet
- Quarter 2 Summative Science TestDocument4 pagesQuarter 2 Summative Science TestSharmaine RamirezNo ratings yet
- Chapter 9, Molecular Structure of DNA and RNADocument65 pagesChapter 9, Molecular Structure of DNA and RNAOmicron TrentNo ratings yet
- Quiz Fungi With AnswerDocument8 pagesQuiz Fungi With AnswerLek SanprasertNo ratings yet
- Clinical Pathway Neonatal PneumoniaDocument4 pagesClinical Pathway Neonatal PneumoniaSHAINA ALIH. JUMAANINo ratings yet
- Answers PGR Week9 2016Document11 pagesAnswers PGR Week9 2016kkk13whyNo ratings yet