You might also like
- Contextual Factors Chart1Document4 pagesContextual Factors Chart1api-213553729No ratings yet
- Comparative Essay: The Sense of Closure in The Endings of A Streetcar Named Desire and Things Fall Apart - Google DocsDocument3 pagesComparative Essay: The Sense of Closure in The Endings of A Streetcar Named Desire and Things Fall Apart - Google DocsLucileNo ratings yet
- Wrights Island Model - Lecture10Document10 pagesWrights Island Model - Lecture10Manikantan KNo ratings yet
- How To Answer A Problematic Question??? Key Points: Topic + I R A C 1) Topic / Scope of DiscussionDocument5 pagesHow To Answer A Problematic Question??? Key Points: Topic + I R A C 1) Topic / Scope of Discussionsyahiir syauqii100% (2)
- Prevalence and Types of AnemiaDocument11 pagesPrevalence and Types of AnemiaRossilawati RachmaNo ratings yet
- PNTD 0007028Document16 pagesPNTD 0007028Gary Elvis TQNo ratings yet
- Malaria Vs DBDDocument9 pagesMalaria Vs DBDade hajizah br ritongaNo ratings yet
- Current Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatesDocument8 pagesCurrent Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatespaulaveronicaNo ratings yet
- 2020 Bidirectional Association Between Tuberculosis and SarcoidosisDocument8 pages2020 Bidirectional Association Between Tuberculosis and SarcoidosisLCCNo ratings yet
- 21, Malaria Vs Dengue 2020Document4 pages21, Malaria Vs Dengue 2020Raquel FernandezNo ratings yet
- 2021 - Acute Chagas Disease in ColombiaDocument14 pages2021 - Acute Chagas Disease in ColombiaDaniel Velázquez-RamírezNo ratings yet
- BR J Haematol - 2020 - Fogarty - COVID19 Coagulopathy in Caucasian PatientsDocument6 pagesBR J Haematol - 2020 - Fogarty - COVID19 Coagulopathy in Caucasian PatientsBarbara BusanelloNo ratings yet
- Undiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDocument6 pagesUndiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDian EsthyNo ratings yet
- International Journal of Health Sciences and Research: A Study of Hematological Profile in HIV/AIDSDocument16 pagesInternational Journal of Health Sciences and Research: A Study of Hematological Profile in HIV/AIDSAnonymous dg1YVnmZ0rNo ratings yet
- Jurnal TBC Inter 1Document5 pagesJurnal TBC Inter 1sekti lindaNo ratings yet
- Case Report: Fatal Staphylococcal Infection Following Classic Dengue FeverDocument4 pagesCase Report: Fatal Staphylococcal Infection Following Classic Dengue FeverRia Septi HarmiaNo ratings yet
- Disseminated Intravascular Coagulation in Patients With 2019Document2 pagesDisseminated Intravascular Coagulation in Patients With 2019Anonymous ps1JIBNo ratings yet
- Association of Iron Deficiency Anemia With Tuberculosis in Taiwan: A Nationwide Population-Based StudyDocument11 pagesAssociation of Iron Deficiency Anemia With Tuberculosis in Taiwan: A Nationwide Population-Based StudyDipyanalarNo ratings yet
- Practiva No 3 Anova Serrano 2017Document7 pagesPractiva No 3 Anova Serrano 2017CARLOS DIONEY MOLINA CLEMENTENo ratings yet
- 33 59 1 SMDocument5 pages33 59 1 SMQobert KEeNo ratings yet
- 1563 6349 1 PBDocument5 pages1563 6349 1 PBwikalydiaprawiraNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- Risk Factors For Mortality in Patients With DengueDocument13 pagesRisk Factors For Mortality in Patients With DengueTaufiqurrokhman RofiiNo ratings yet
- PJMS 38 1968Document5 pagesPJMS 38 1968Mila KarmilaNo ratings yet
- High Prevalence of Pneumocystis Jirovecii Pneumonia Among Mozambican Children 5 Years of Age Admitted To Hospital With Clinical Severe PneumoniaDocument7 pagesHigh Prevalence of Pneumocystis Jirovecii Pneumonia Among Mozambican Children 5 Years of Age Admitted To Hospital With Clinical Severe PneumoniaAnonymous qpHeArUNo ratings yet
- Characteristics of Peripheral Blood Differential Counts in Hospitalized Patients With COVID-19Document6 pagesCharacteristics of Peripheral Blood Differential Counts in Hospitalized Patients With COVID-19cika daraNo ratings yet
- Hematology Profile of Tuberculosis Lymphadenitis Patients at Siti Rahmah Hospital, Padang, IndonesiaDocument5 pagesHematology Profile of Tuberculosis Lymphadenitis Patients at Siti Rahmah Hospital, Padang, IndonesiaNofiana AyuNo ratings yet
- TB and PADDocument7 pagesTB and PADdicky wahyudiNo ratings yet
- Pancytopenia in Children: Etiological ProfileDocument4 pagesPancytopenia in Children: Etiological ProfileHanshel SatriyaNo ratings yet
- Impact of Blood Group in Dengue: A Study: Original Research ArticleDocument5 pagesImpact of Blood Group in Dengue: A Study: Original Research ArticleMuhammad AfzaalNo ratings yet
- Transient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsDocument10 pagesTransient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsNura RamadhanNo ratings yet
- Prokalsitonin Dan Kultur Darah Sebagai Penanda Sepsis Di Rsup DR Wahidin Sudirohusodo MakassarDocument11 pagesProkalsitonin Dan Kultur Darah Sebagai Penanda Sepsis Di Rsup DR Wahidin Sudirohusodo MakassarAnonymous ORleRrNo ratings yet
- Prevalence of diabetes among tuberculosis patients in GuyanaDocument4 pagesPrevalence of diabetes among tuberculosis patients in GuyanaAgungBudiPamungkasNo ratings yet
- Declining Case Fatality Rates For Severe Sepsis Good Data Bring Good News With Ambiguous ImplicationsDocument3 pagesDeclining Case Fatality Rates For Severe Sepsis Good Data Bring Good News With Ambiguous ImplicationsRodrigoSachiFreitasNo ratings yet
- 4Document16 pages4Ihsanul Ma'arifNo ratings yet
- Dengue_in_Renal_Transplant_Patients_A_ReDocument3 pagesDengue_in_Renal_Transplant_Patients_A_ReMaira EscobarNo ratings yet
- Journal Pone 0252599Document12 pagesJournal Pone 0252599sririniaNo ratings yet
- Review Jurnal BIOMOLDocument16 pagesReview Jurnal BIOMOLaulia fauziyahahNo ratings yet
- Clinical Presentation and Bacterial Etiology of Adult Community Acquired PneumoniaDocument7 pagesClinical Presentation and Bacterial Etiology of Adult Community Acquired PneumonialyaNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- HIV Resistance in Patients With Sickle Cell AnaemiaDocument3 pagesHIV Resistance in Patients With Sickle Cell AnaemiaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Lopez 2021Document14 pagesLopez 2021Roger CalderonNo ratings yet
- 1 s2.0 S0735675721002709 MainDocument8 pages1 s2.0 S0735675721002709 MainAji SadamNo ratings yet
- ABO Blood Type Association With SARS CoV 2 Infection Mortality 2021Document7 pagesABO Blood Type Association With SARS CoV 2 Infection Mortality 2021azizk83No ratings yet
- Anemia and Thrombocytopenia in People Living With HIV AIDSDocument12 pagesAnemia and Thrombocytopenia in People Living With HIV AIDSAngga SantosaNo ratings yet
- Terapi TBDocument11 pagesTerapi TBAdy WarsanaNo ratings yet
- Sepsis Proposal1Document34 pagesSepsis Proposal1Appiah Peter OforiNo ratings yet
- 100220080112Document8 pages100220080112Nabil MrhiliNo ratings yet
- NEJM - Sickle Cell Disease PDFDocument13 pagesNEJM - Sickle Cell Disease PDFHumberto BritoNo ratings yet
- The Changing Epidemiology of Invasive Fungal InfectionsDocument49 pagesThe Changing Epidemiology of Invasive Fungal InfectionsHèla HassenNo ratings yet
- COVID-19 in People With Diabetes: Urgently Needed Lessons From Early ReportsDocument4 pagesCOVID-19 in People With Diabetes: Urgently Needed Lessons From Early ReportsIndahNo ratings yet
- Yogaraj 2002Document7 pagesYogaraj 2002زينب محمد عبدNo ratings yet
- Makale 4Document7 pagesMakale 4meuaciltipNo ratings yet
- Ficha 5Document12 pagesFicha 5mariaNo ratings yet
- News & Views: CKD Is A Key Risk Factor For COVID-19 MortalityDocument2 pagesNews & Views: CKD Is A Key Risk Factor For COVID-19 Mortalityrini trismiatiNo ratings yet
- PIIS0022510X20304998Document7 pagesPIIS0022510X20304998dhea handyaraNo ratings yet
- Neutropenic Colitis in Children 2011Document4 pagesNeutropenic Colitis in Children 2011IRINA SULEY TIRADO PEREZNo ratings yet
- Necrotizing Fasciitis: A Six-Year ExperienceDocument8 pagesNecrotizing Fasciitis: A Six-Year Experiencepjanu86No ratings yet
- 2016 Article 1668Document7 pages2016 Article 1668Rahmiati LaoNo ratings yet
- 1 s2.0 S0022316622028917 MainDocument8 pages1 s2.0 S0022316622028917 MainRafi DaniswaraNo ratings yet
- Aos 13961Document8 pagesAos 13961Vivian Ayte LopezNo ratings yet
- Infectious Diseases: Ratio of Monocytes To Lymphocytes in Peripheral Blood in Patients Diagnosed With Active TuberculosisDocument7 pagesInfectious Diseases: Ratio of Monocytes To Lymphocytes in Peripheral Blood in Patients Diagnosed With Active TuberculosisMario GintingNo ratings yet
- Babesiosis in Pregnancy: An Imitator of HELLP SyndromeDocument6 pagesBabesiosis in Pregnancy: An Imitator of HELLP Syndromemade dharmaNo ratings yet
- The War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersFrom EverandThe War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersNo ratings yet
- Whole Genome Sequencing Mycobacterium Tuberculosis Directly From Sputum Identifies More Genetic Diversity Than Sequencing From CultureDocument9 pagesWhole Genome Sequencing Mycobacterium Tuberculosis Directly From Sputum Identifies More Genetic Diversity Than Sequencing From CultureidhaNo ratings yet
- Studying Public Perception About Vaccination: A Sentiment Analysis of TweetsDocument23 pagesStudying Public Perception About Vaccination: A Sentiment Analysis of TweetsidhaNo ratings yet
- Review - New Drugs, Treatment and HDTs THELANCETID-S-17-01880Document49 pagesReview - New Drugs, Treatment and HDTs THELANCETID-S-17-01880idhaNo ratings yet
- Jurnal Sigid - Nur - Itto 2016Document19 pagesJurnal Sigid - Nur - Itto 2016idhaNo ratings yet
- EJMCM - Volume 7 - Issue 7 - Pages 1157-1165Document9 pagesEJMCM - Volume 7 - Issue 7 - Pages 1157-1165idhaNo ratings yet
- Mycobacterium TuberculosisDocument11 pagesMycobacterium TuberculosisidhaNo ratings yet
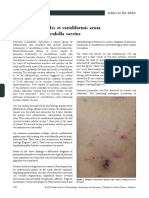
- Pityriasis Lichenoides Et Varioliformis Acuta Following Measles Rubella VaccineDocument3 pagesPityriasis Lichenoides Et Varioliformis Acuta Following Measles Rubella VaccineidhaNo ratings yet
- NIH Public AccessDocument6 pagesNIH Public AccessidhaNo ratings yet
- Undernutrition and Treatment Success in Drug-Resistant Tuberculosis in UgandaDocument9 pagesUndernutrition and Treatment Success in Drug-Resistant Tuberculosis in UgandaidhaNo ratings yet
- Sociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaDocument4 pagesSociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaidhaNo ratings yet
- A Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionDocument7 pagesA Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionidhaNo ratings yet
- Rumah Impian: My Little FamilyDocument1 pageRumah Impian: My Little FamilyidhaNo ratings yet
- ACross sectionalStudyofMorphologicalTypesofAnemiainPulmonaryTuberculosisPatientandAssociatedRiskDocument7 pagesACross sectionalStudyofMorphologicalTypesofAnemiainPulmonaryTuberculosisPatientandAssociatedRiskidhaNo ratings yet
- Clinical Microbiology and Infection: M.L. WilsonDocument6 pagesClinical Microbiology and Infection: M.L. WilsonidhaNo ratings yet
- Genomics: MinireviewDocument4 pagesGenomics: MinireviewidhaNo ratings yet
- Update On The Virulence Factors of The Obligate Pathogen Mycobacterium Tuberculosis and Related Tuberculosis-Causing MycobacteriaDocument32 pagesUpdate On The Virulence Factors of The Obligate Pathogen Mycobacterium Tuberculosis and Related Tuberculosis-Causing MycobacteriaidhaNo ratings yet
- Arbovirus & Rodent-Borne S2 IKT NOV 2016Document54 pagesArbovirus & Rodent-Borne S2 IKT NOV 2016idhaNo ratings yet
- Character & Life Cycle of MicrobesDocument35 pagesCharacter & Life Cycle of MicrobesidhaNo ratings yet
- GrammarDocument10 pagesGrammarRidhan RahmahNo ratings yet
- Amity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatDocument10 pagesAmity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatYash TiwariNo ratings yet
- 206841Document1 page206841VinceOnikaa PerryGermanottaNo ratings yet
- Architecture Statement of PurposeDocument4 pagesArchitecture Statement of PurposeAZAR HOSNo ratings yet
- Comparison Surgical Lengthening: Clinical of Desired Versus Actual Amount of CrownDocument4 pagesComparison Surgical Lengthening: Clinical of Desired Versus Actual Amount of CrownOana DimaNo ratings yet
- RitzeDocument4 pagesRitzeLalai IskolatongNo ratings yet
- F&P Level IndicatorsDocument23 pagesF&P Level IndicatorsBen100% (1)
- Academic Literacy Skills for Science PortfolioDocument71 pagesAcademic Literacy Skills for Science PortfolioUshari I.K. EgodaweleNo ratings yet
- What Makes A Family Strong and Successful?Document1 pageWhat Makes A Family Strong and Successful?Chinmayee SrivathsaNo ratings yet
- Supreme Court Detailed Judgement On Asia Bibi's AppealDocument56 pagesSupreme Court Detailed Judgement On Asia Bibi's AppealDawndotcom94% (35)
- Past-Simple-Regular-Verbs - WORD (Falta)Document21 pagesPast-Simple-Regular-Verbs - WORD (Falta)jeinNo ratings yet
- Form: Contours and Areas V: Stefan ArteniDocument100 pagesForm: Contours and Areas V: Stefan Artenistefan arteniNo ratings yet
- Forensic Dentistry Case Book 6:: A Self-Inflicted Bite Mark A Case ReportDocument2 pagesForensic Dentistry Case Book 6:: A Self-Inflicted Bite Mark A Case ReportRizky Mega ChandraNo ratings yet
- MOU Khusboo & NitishDocument4 pagesMOU Khusboo & NitishRimika ChauhanNo ratings yet
- Audit of Receivables Pre-Assessment: Acctg35Document3 pagesAudit of Receivables Pre-Assessment: Acctg35Jeane Mae BooNo ratings yet
- SHCT 167 Reeves - English Evangelicals and Tudor Obedience, C. 1527-1570 2013 PDFDocument222 pagesSHCT 167 Reeves - English Evangelicals and Tudor Obedience, C. 1527-1570 2013 PDFL'uomo della Rinascitá100% (1)
- Reference: A Visual Dictionary By: D.K. Ching: ArchitectureDocument75 pagesReference: A Visual Dictionary By: D.K. Ching: ArchitectureRemzskie PaduganaoNo ratings yet
- THE ENNEAGRAM: A TOOL FOR GOING BENEATH THE SURFACEDocument9 pagesTHE ENNEAGRAM: A TOOL FOR GOING BENEATH THE SURFACEsecretofkellysNo ratings yet
- Activity Guide and Evaluation Rubric - Activity 7 - Creating A WIX PageDocument5 pagesActivity Guide and Evaluation Rubric - Activity 7 - Creating A WIX PageLina VergaraNo ratings yet
- ISO 9001:2015 certified Fargo Courier with over 100 branchesDocument1 pageISO 9001:2015 certified Fargo Courier with over 100 branchesMuchiri NahashonNo ratings yet
- Hybrid - 01Document209 pagesHybrid - 01Santos ArwinNo ratings yet
- Types of Communication Networks - StudytonightDocument10 pagesTypes of Communication Networks - StudytonightHAMEED ULLAHNo ratings yet
- A Case Study of A Turnaround PrincipalDocument7 pagesA Case Study of A Turnaround PrincipalReynante Roxas MalanoNo ratings yet
- Military Organization of the Anglo-Saxon FyrdDocument24 pagesMilitary Organization of the Anglo-Saxon FyrdMiguel TrindadeNo ratings yet
- Mastery-Test-Math-10-Quarter-3 Week 5-6Document1 pageMastery-Test-Math-10-Quarter-3 Week 5-6Sheila Mauricio GarciaNo ratings yet
- Basic Calculus L2Document14 pagesBasic Calculus L2Abbie MalutoNo ratings yet