Articles
Efficacy and safety of the CVnCoV SARS-CoV-2 mRNA vaccine
candidate in ten countries in Europe and Latin America
(HERALD): a randomised, observer-blinded,
placebo-controlled, phase 2b/3 trial
Peter G Kremsner*, Rodolfo Andrés Ahuad Guerrero, Eunate Arana-Arri, Gustavo Jose Aroca Martinez, Marc Bonten, Reynaldo Chandler,
Gonzalo Corral, Eddie Jan Louis De Block, Lucie Ecker, Julian Justin Gabor, Carlos Alberto Garcia Lopez, Lucy Gonzales,
María Angélica Granados González, Nestor Gorini, Martin P Grobusch, Adrian D Hrabar, Helga Junker, Alan Kimura, Claudio F Lanata,
Clara Lehmann, Isabel Leroux-Roels, Philipp Mann, Michel Fernando Martinez-Reséndez, Theresa J Ochoa, Carlos Alberto Poy,
Maria Jose Reyes Fentanes, Luis Maria Rivera Mejia, Vida Veronica Ruiz Herrera, Xavier Sáez-Llorens, Oliver Schönborn-Kellenberger,
Mirjam Schunk, Alexandra Sierra Garcia, Itziar Vergara, Thomas Verstraeten, Marisa Vico, Lidia Oostvogels*, on behalf of the
HERALD Study Group†
Summary
Background Additional safe and efficacious vaccines are needed to control the COVID-19 pandemic. We aimed to Lancet Infect Dis 2021
analyse the efficacy and safety of the CVnCoV SARS-CoV-2 mRNA vaccine candidate. Published Online
November 23, 2021
https://doi.org/10.1016/
Methods HERALD is a randomised, observer-blinded, placebo-controlled, phase 2b/3 clinical trial conducted in
S1473-3099(21)00677-0
47 centres in ten countries in Europe and Latin America. By use of an interactive web response system and
See Online/Comment
stratification by country and age group (18–60 years and ≥61 years), adults with no history of virologically confirmed https://doi.org/10.1016/
COVID-19 were randomly assigned (1:1) to receive intramuscularly either two 0·6 mL doses of CVnCoV containing S1473-3099(21)00687-3
12 μg of mRNA or two 0·6 mL doses of 0·9% NaCl (placebo) on days 1 and 29. The primary efficacy endpoint was the *Authors are listed
occurrence of a first episode of virologically confirmed symptomatic COVID-19 of any severity and caused by any alphabetically, except for the
strain from 15 days after the second dose. For the primary endpoint, the trial was considered successful if the lower first and last author
limit of the CI was greater than 30%. Key secondary endpoints were the occurrence of a first episode of virologically †Members are listed in the
appendix (p 3)
confirmed moderate-to-severe COVID-19, severe COVID-19, and COVID-19 of any severity by age group. Primary
Institute of Tropical Medicine,
safety outcomes were solicited local and systemic adverse events within 7 days after each dose and unsolicited adverse
University of Tübingen,
events within 28 days after each dose in phase 2b participants, and serious adverse events and adverse events of Tübingen, Germany
special interest up to 1 year after the second dose in phase 2b and phase 3 participants. Here, we report data up to (Prof P G Kremsner MD,
June 18, 2021. The study is registered at ClinicalTrials.gov, NCT04652102, and EudraCT, 2020–003998–22, J J Gabor MD); Centre de
Recherches Médicales de
and is ongoing. Lambaréné, Lambaréné, Gabon
(Prof P G Kremsner,
Findings Between Dec 11, 2020, and April 12, 2021, 39 680 participants were enrolled and randomly assigned to receive Prof M P Grobusch FRCP);
either CVnCoV (n=19 846) or placebo (n=19 834), of whom 19 783 received at least one dose of CVnCoV and German Center for Infection
Research, Tübingen, Germany
19 746 received at least one dose of placebo. After a mean observation period of 48·2 days (SE 0·2), 83 cases of (Prof P G Kremsner,
COVID-19 occurred in the CVnCoV group (n=12 851) in 1735·29 person-years and 145 cases occurred in the placebo Prof M P Grobusch); Corporacion
group (n=12 211) in 1569·87 person-years, resulting in an overall vaccine efficacy against symptomatic COVID-19 of Medica de General San Martin,
48·2% (95·826% CI 31·0–61·4; p=0·016). Vaccine efficacy against moderate-to-severe COVID-19 was 70·7% (95% CI Buenos Aires, Argentina
(R A Ahuad Guerrero MD);
42·5–86·1; CVnCoV 12 cases in 1735·29 person-years, placebo 37 cases in 1569·87 person-years). In participants Biocruces Health Research
aged 18–60 years, vaccine efficacy against symptomatic disease was 52·5% (95% CI 36·2–64·8; CVnCoV 71 cases in Institute, Barakaldo, Bizkaia,
1591·47 person-years, placebo, 136 cases in 1449·23 person-years). Too few cases occurred in participants aged Spain (E Arana-Arri PhD);
61 years or older (CVnCoV 12, placebo nine) to allow meaningful assessment of vaccine efficacy. Solicited adverse Scientific Coordination Unit,
Cruces University Hospital,
events, which were mostly systemic, were more common in CVnCoV recipients (1933 [96·5%] of 2003) than in Osakidetza, Barakaldo, Spain
placebo recipients (1344 [67·9%] of 1978), with 542 (27·1%) CVnCoV recipients and 61 (3·1%) placebo recipients (E Arana-Arri); Postgraduate
reporting grade 3 solicited adverse events. The most frequently reported local reaction after any dose in the CVnCoV School of Nephrology,
group was injection-site pain (1678 [83·6%] of 2007), with 22 grade 3 reactions, and the most frequently reported Clínica de la Costa y
Universidad Simón Bolívar,
systematic reactions were fatigue (1603 [80·0%] of 2003) and headache (1541 [76·9%] of 2003). 82 (0·4%) of Barranquilla, Colombia
19 783 CVnCoV recipients reported 100 serious adverse events and 66 (0·3%) of 19 746 placebo recipients reported (G J Aroca Martinez MD); Julius
76 serious adverse events. Eight serious adverse events in five CVnCoV recipients and two serious adverse events in Center for Health Sciences and
Primary Care, UMC Utrecht,
two placebo recipients were considered vaccination-related. None of the fatal serious adverse events reported (eight in
Utrecht University,
the CVnCoV group and six in the placebo group) were considered to be related to study vaccination. Adverse events of Utrecht, Netherlands
special interest were reported for 38 (0·2%) participants in the CVnCoV group and 31 (0·2%) participants in the (Prof M Bonten MD); Cevaxin,
placebo group. These events were considered to be related to the trial vaccine for 14 (<0·1%) participants in the Panama City, Panama
(R Chandler MD); Instituto de
CVnCoV group and for five (<0·1%) participants in the placebo group.
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 1
Articles
Investigaciones Clinicas de Mar Interpretation CVnCoV was efficacious in the prevention of COVID-19 of any severity and had an acceptable safety
del Plata, Mar del Plata, profile. Taking into account the changing environment, including the emergence of SARS-CoV-2 variants, and
Argentina (G Corral MD);
Cohezio, Brussels, Belgium
timelines for further development, the decision has been made to cease activities on the CVnCoV candidate and to
(E J L De Block MD); Instituto de focus efforts on the development of next-generation vaccine candidates.
Investigación Nutricional,
Lima, Peru (L Ecker MD, Funding German Federal Ministry of Education and Research and CureVac.
Prof C F Lanata MD); Unidad de
Medicina Especializada,
San Juan del Río, Mexico Copyright © 2021 Elsevier Ltd. All rights reserved.
(C A Garcia Lopez MD); Clinica
Medica San Martin, Ica, Peru Introduction humans in Europe and the USA on the basis of data
(L Gonzales MD); Centro de
Atención e Investigación
SARS-CoV-2, which emerged in China’s Wuhan province from phase 3 efficacy trials.7,8
Médica, Bogotá, Colombia in December, 2019, has led to more than 225 million cases CVnCoV is a chemically unmodified mRNA vaccine
(M A Granados González MSc); of COVID-19 and more than 4·5 million deaths globally candidate based on the RNActive mRNA vaccine platform
Haematology and as of September, 2021.1 Through unprecedented effort encoding the stabilised, full-length, native SARS-CoV-2
Haemotherapy Diagnosis
and Treatment Unit, Hospital
from governments, national and international research spike protein of the SARS-CoV-2 wild-type strain. The
Zonal General de Agudos funders, regulatory bodies, and research organisations, mRNA is protected by lipid nanoparticles used for delivery.
Descentralizado Evita Pueblo vaccine development has been, and continues to be, Preclinical studies have shown that CVnCoV induces a
de Berazategui, Buenos Aires,
expedited. The first conditionally approved vaccine in robust immune response and protects against SARS-CoV-2
Argentina (N Gorini MD);
Center of Tropical Medicine and Europe was administered in December, 2020, within in hamster and primate virus challenge models.9,10 In
Travel Medicine, Department 9 months of WHO characterising COVID-19 as a a phase 1 dose-escalation study, two doses of CVnCoV
of Infectious Diseases, pandemic on March 11, 2020.2 administered 28 days apart were safe and immunogenic,
Amsterdam University Medical
More than 100 COVID-19 vaccines are currently in with dose-dependent increases in anti-spike protein
Center, Amsterdam Public
Health, Amsterdam clinical development, and as of September, 2021, 21 are IgG antibodies and SARS-CoV-2-neutralising antibodies.11
Infection and Immunity, being offered to the general population.3 These vaccines Median antibody titres against spike protein and its
University of Amsterdam, have been developed by use of different platforms, receptor binding domain after two 12 μg doses of CVnCoV
Amsterdam, Netherlands
all with specific advantages and disadvantages.4 were similar to those observed in convalescent serum
(Prof M P Grobusch); Instituto
de Investigaciones Clínicas mRNA is a promising platform that allows the rapid samples from patients with COVID-19, with seroc
Quilmes, Hudson, Argentina development of immunogens and vaccine production.5,6 onversion observed 2 weeks after the second dose in all
(A D Hrabar MD); CureVac, The BNT162b2 (Pfizer-BioNtech) and mRNA-1273 participants receiving this dosage. On the basis of these
Tübingen, Germany
(Moderna) SARS-CoV-2 vaccines were the first mRNA findings, the 12 μg dose was selected for further phase 2/3
(H Junker MD, A Kimura MD,
P Mann MD, L Oostvogels MD); preventive vaccines to be approved for emergency use in testing. We aimed to analyse the efficacy and safety of the
School of Medicine, Vanderbilt
University, Nashville, TN, USA
Research in context
(Prof C F Lanata); Department
of Epidemiology, London
Evidence before this study adverse events were common, and more frequently reported in
School of Hygiene & Tropical
Medicine, London, UK We searched PubMed for clinical trials published between the CVnCoV group than in the placebo group, but the median
(Prof C F Lanata); Infection Jan 1, 2019, and Sept 19, 2021, without language restrictions, duration of grade 3 solicited adverse events was 1 day. CVnCoV
Protection Centre (ISZ) & using the terms ’SARS-CoV-2’ OR ’COVID-19’ AND ’Vaccine’ was 48·2% efficacious in the prevention of COVID-19 of any
Infection Outpatient Clinic,
AND ’Efficacy’. At the time of the search, we identified 12 peer- severity in a variant-dominated setting. Indeed, only seven (3%)
Innere Medizin I, Uniklinik
Köln, Cologne, Germany reviewed publications of phase 2/3 and phase 3 clinical trials of all 204 sequenced COVID-19 cases were of B.1 lineage, with the
(Prof C Lehmann MD); Center reporting the efficacy of COVID-19 vaccines in different others caused by 14 different variants. In Europe, 45 (92%) of
for Vaccinology, Ghent populations. We did not consider press releases or preprints as 49 cases were caused by the alpha variant of concern (B.1.1.7),
University Hospital, Ghent,
sources of information. Eight primary publications reported compared with Latin America where 20 (13%) of 155 cases were
Belgium (I Leroux-Roels MD);
School of Medicine and Health vaccine efficacies ranging from 62% to 95%. The mRNA-1273 caused by the alpha variant and 35 (23%) cases were caused by
Sciences, Tecnologico de (Moderna) and BNT162b2 (Pfizer-BioNtech) mRNA vaccines the gamma variant of concern (P.1).
Monterrey, Monterrey, Mexico have shown 94% and 95% efficacy, respectively, in preventing
(M F Martinez-Reséndez MD); Implications of all the available evidence
COVID-19, with cases accrued at a time when no circulating
Instituto de Medicina Tropical In view of the changing environment, including the emergence
Alexander von Humboldt variants had been identified. Variant-dependent differences in
of SARS-CoV-2 variants, and taking into account timelines for
(T J Ochoa MD) and Facultad de vaccine efficacy have been reported, with reductions in efficacy
Medicina (T J Ochoa), further development, the decision has been made to cease
of up to 60 percentage points against newly emerged
Universidad Peruana Cayetano activities on the CVnCoV candidate and to focus efforts on the
SARS-CoV-2 variants of concern.
Heredia, Lima, Peru; Center for promising and rapidly progressing development of next-
Infectious Diseases, School of
Added value of this study generation vaccine candidates. In addition, it might be
Public Health, University of
Texas Health Science Center at We report the primary efficacy analysis of the CVnCoV mRNA necessary to consider alternative designs for future global
Houston, Houston, TX, USA vaccine candidate from the phase 2b/3 HERALD trial that efficacy trials given the number of rapidly emerging
(T J Ochoa); Sanatorio Parque, comprised 39 680 participants from ten countries in Europe and SARS-CoV-2 variants and the high uptake of COVID-19 vaccines
Rosario, Argentina
Latin America. CVnCoV had an acceptable safety profile. Solicited under emergency use authorisation.
(C A Poy MD); PanAmerican
2 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
Articles
CVnCoV SARS-CoV-2 mRNA vaccine candidate in a committees or institutional review boards at each study Clinical Research México,
phase 2b/3 trial. centre. The trial is being conducted in accordance with Juriquilla, Mexico
(M J Reyes Fentanes MD);
the provisions of the Declaration of Helsinki and Fundacion Dominicana de
Methods the International Conference on Harmonisation Good Perinatologia, Hospital
Study design and participants Clinical Practice guidelines. All participants provided Universitario Maternidad
HERALD is an ongoing, randomised, observer-blinded, written informed consent before initiation of any trial Nuestra Senora de la
Altagracia, Santo Domingo,
placebo-controlled, phase 2b/3, clinical trial in procedures. Dominican Republic
47 public and private hospitals and clinics across (Prof L M Rivera Mejia MD);
four countries in Europe (ie, Belgium, Germany, Randomisation and masking PanAmerican Clinical Research,
Guadalajara, Mexico
the Netherlands, and Spain) and six countries in Trial participants were randomly assigned (1:1) to receive
(V V Ruiz Herrera MD); Clinical
Latin America (ie, Argentina, Colombia, Dominican either CVnCoV or placebo. Randomisation, stratified by Research Department,
Republic, Mexico, Panama, and Peru). Participants were country and age group (18–60 years and ≥61 years), was Panama City, Panama
recruited by study sites through their databases and done centrally by use of an interactive web response (X Sáez-Llorens MD); Cevaxin
Research Center, Panama City,
advertisements. Adults aged 18 years or older with no system. The randomisation scheme was generated
Panama (X Sáez-Llorens);
history of virologically confirmed COVID-19 were eligible and managed by an independent statistics group at Senacyt, Panama City, Panama
for inclusion, unless they had received (within 28 days the contract research organisation, PRA. Due to the (X Sáez-Llorens); Cogitars,
before first administration of CVnCoV), or planned to difference in appearance and presentation between the Heidelberg, Germany
(O Schönborn-Kellenberger MSc);
receive, any investigational or non-registered vaccine or CVnCoV vaccine candidate and placebo, site personnel
Division of Infectious Diseases
drug; had received any live (within 28 days) or inactivated involved in preparing the vaccine masked the content of and Tropical Medicine, LMU
(within 14 days) vaccine; or had received, or planned to the syringe with a label and were not involved in further Klinikum, Munich, Germany
receive, any investigational SARS-CoV-2 vaccine or other conduct of the trial. Investigators, site personnel, and (M Schunk MD); Centro de
estudios en Infectologia
coronavirus vaccine before trial initiation or during the others directly involved in the conduct of the trial were
Pediatrica, Cali, Colombia
trial. A list of all inclusion and exclusion criteria is masked to participant allocation for the duration of the (A Sierra Garcia MD); Primary
provided in the appendix (p 4). Eligibility could be trial. The statisticians analysing the data were masked to Care Group, Biodonostia
assessed and recording of baseline data could be done up group assignment until the final analyses. Unmasking of Institute for Health Research,
Donostia-San Sebastián, Spain
to 21 days before administration of the trial vaccine, but participants was allowed in emergency situations for (I Vergara PhD); Research
had to be reviewed before administration on day 1. reasons of participant safety or for participants who Network in Health Services in
The initial phase 2b part of the trial was designed to became eligible to receive an authorised SARS-CoV-2 Chronic Diseases, Baracaldo,
characterise the safety, reactogenicity, and immuno vaccine and requested unmasking. Spain (I Vergara); P95
Pharmacovigilance and
genicity of the CVnCoV vaccine candidate, and the Epidemiology Services, Leuven,
phase 3 part of the trial was designed to evaluate its Procedures Belgium (T Verstraeten MD);
efficacy and safety. The two parts of the trial were designed Participants in both the phase 2b and the phase 3 parts of Instituto de Investigaciones
to allow participants with COVID-19 accrued in the the trial received either two 0·6 mL doses of CVnCoV Clínicas Zárate, Buenos Aires,
Argentina (M Vico MD)
phase 2b part of the trial to be pooled with those in the containing 12 μg of mRNA, formulated with the RNActive
Correspondence to:
phase 3 part of the trial for the primary analysis of vaccine mRNA vaccine platform, or two 0·6 mL doses of 0·9% Prof Peter G Kremsner, Institute
efficacy. An independent data and safety monitoring NaCl (placebo) on days 1 and 29. Each 0·6 mL dose was of Tropical Medicine, University
board (DSMB) conducted interim safety reviews of the administered by intramuscular injection in the deltoid of Tübingen, Tübingen 72074,
phase 2b part of the trial before enrolment for the phase 3 area. Blood samples (6 mL) were taken from all Germany
peter.kremsner@uni-
part of the trial was initiated and will continue to monitor participants on day 1 and day 43 (14 days after the second tuebingen.de
safety until study end. An enrolment target was that dose) and will be taken on day 211 and day 393 (study end)
See Online for appendix
20–25% of the population would be aged 61 years or older. to measure SARS-CoV-2 nucleocapsid protein serostatus.
We planned to enrol the first 4000 participants in the The samples were sent to one of two central laboratories
phase 2b part of the trial and to include the first in the USA or the Netherlands and tested with the Elecsys
600 participants in each age group in the assessment of assay on the COBAS system (Roche Diagnostics;
immunogenicity endpoints. The DSMB reviewed the Mannheim, Germany). The results on day 1 and day 43
safety data when approximately 1800 participants (900 in identified whether participants were naive to SARS-CoV-2
both treatment groups) had been enrolled in the phase 2b infection at trial entry and 15 days after the second
part of the trial and had at least 1 week of safety follow-up vaccination, and were therefore eligible for inclusion in
after the first dose. Enrolment of participants into the the efficacy analysis subset.
phase 3 part of the trial would begin without interruption Participants were requested to contact site investigators
from the phase 2b part of the trial if the safety profile was if they had symptoms potentially indicating COVID-19
considered acceptable. The DSMB also reviewed all safety (eg, fever or chills, cough, shortness of breath or difficulty
data after all participants in each group in the phase 2b breathing, fatigue, muscle or body aches, headache, new
trial had received their second trial vaccination and had at loss of taste or smell, sore throat, congestion or runny
least 1 week of safety follow-up. nose, nausea or vomiting, or diarrhoea),12 and participants
The trial protocol and its amendments received ethics were contacted twice per week by site staff via a mobile
approval from the appropriate independent ethics application to respond yes or no to having potential
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 3
Articles
COVID-19 symptoms. Site personnel then contacted Illumina Next Generation Sequencing (Viracor-Eurofins,
participants who replied yes to ascertain whether their Lee’s Summit, MO, USA).
symptoms were indicative of COVID-19 by following a Mild COVID-19 was defined as disease without shortness
scripted interview. Upon suspicion of COVID-19, of breath or difficulty breathing, and an altitude-adjusted
participants underwent a rapid antigen test (Abbott oxygen saturation (SpO2) of at least 95%. Moderate disease
Panbio COVID-19 Ag Rapid Test; Jena, Germany) to was defined by the presence of symptoms and shortness
allow them to comply with local quarantine rules if the of breath, difficulty breathing, a respiratory rate of
results were positive. In addition, samples were 20–29 breaths per min, abnormal SpO2 (but still >93%
sent to central laboratories for SARS-CoV-2-specific when adjusted for altitude), clinical or radiographic
RT-PCR testing (In-house test, with probes and primers evidence of lower respiratory tract disease, or radiological
from Eurofins [Louisville KY, USA]; Latin America evidence of deep vein thrombosis. Severe COVID-19 was
testing done in Lancaster [PA, USA]; European testing defined by clinical signs at rest that are indicative of severe
done in Breda [Netherlands]) for virological confirmation systemic illness (respiratory rate ≥30 breaths per min, heart
of COVID-19. In case of discrepancies between tests, the rate ≥125 beats per min, altitude-adjusted SpO2 ≤93%, or
RT-PCR test result was considered definitive. All primary PaO2/FiO2 ratio <300 mmHg), respiratory failure, evidence
efficacy cases were confirmed by an independent of shock, considerable renal, hepatic, or neurological
adjudication committee. Sequencing of the complete dysfunction, admission to an intensive care unit, or death.13
viral single stranded RNA genome was carried out using The phase 2b participants used a diary to record
solicited local adverse events (ie, injection-site pain,
redness, swelling, and itching) and solicited systemic
42 266 individuals screened for eligibility adverse events (ie, fever, headache, fatigue, chills,
myalgia, arthralgia, nausea or vomiting, and diarrhoea)
for 7 days after each dose. Solicited adverse events were
2586 ineligible
graded by intensity from 0 (absent) to 3 (severe) according
to predefined criteria provided in the appendix (p 5).
39 680 enrolled Unsolicited adverse events were recorded in the diaries
for 28 days after each dose, and investigators assessed
their severity.
39 680 randomised
Medically attended adverse events will be collected for
all participants from day 1 until 6 months after the
second dose. Adverse events of special interest and
19 846 assigned CVnCoV 19 834 assigned placebo serious adverse events will be collected until 1 year after
the second dose. A list of adverse events of special
interest is provided in the appendix (pp 6–7). The
63 did not receive first dose 88 did not receive first dose
intensity of unsolicited adverse events, adverse events of
special interest, and serious adverse events, and their
19 783 received first dose (including 13 assigned to 19 746 received first dose (including 7 assigned to relationship to study vaccination, were assessed by the
placebo) CVnCoV) study investigators.
353 did not receive second dose 1269 did not receive second dose Outcomes
135 participant decision 541 participant decision The primary efficacy outcome was the occurrence of a first
42 SARS-CoV-2 infection 63 SARS-CoV-2 infection
23 adverse event 18 adverse event episode of virologically confirmed symptomatic COVID-19
21 physician decision 73 physician decision of any severity and caused by any strain from 15 days after
9 protocol deviation 14 protocol deviation
5 pregnancy 9 pregnancy
the second dose up to 1 year. The primary outcome was
2 died 4 died assessed by a blinded, central adjudication committee. Key
36 no information 68 no information secondary efficacy outcomes included the occurrence of a
80 other 479 other
first episode of virologically confirmed moderate-to-severe
COVID-19, and the occurrence of a first episode of
19 430 received second dose (including 23 assigned 18 477 received second dose (including 10 assigned
virologically confirmed severe COVID-19, overall and by
to placebo) to CVnCoV) age group (18–60 years vs ≥61 years). An exploratory
efficacy endpoint, which was added in the protocol
amendment on March 29, 2021, was the occurrence of a
19 376 in the study as of June 18, 2021 16 158 in the study as of June 18, 2021
first episode of virologically confirmed COVID-19 caused
by an individual variant of concern or interest.
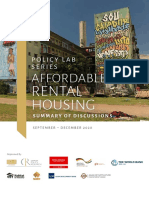
Figure 1: Trial profile for the HERALD phase 2b–3 study
25 participants who were randomly assigned to placebo received at least one dose of CVnCoV, and six participants Primary safety outcomes were the monitoring of
who were randomly assigned to CVnCoV received two doses of placebo; they were analysed according to the solicited local and systemic adverse events for 7 days after
treatment received. The reasons for discontinuing treatment or the study are summarised in the appendix (p 7). each dose and unsolicited adverse events for 28 days after
4 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
Articles
each dose in phase 2b participants, medically attended
CVnCoV (n=19 783) Placebo (n=19 746)
adverse events (which will be reported in the final
analysis at study end) up to 6 months after the second Characteristic
dose, serious adverse events and adverse events of special Sex
interest up to 1 year after the second dose, fatal serious Female 8923 (45·1%) 8934 (45·2%)
adverse events up to 1 year after the second dose, and Male 10 860 (54·9%) 10 812 (54·8%)
adverse events leading to vaccine withdrawal or trial Age, years 43·0 (31·0–54·0) 43·0 (31·0–54·0)
discontinuation for 1 year after the second dose (which 18–60 years 17 277 (87·3%) 17 248 (87·3%)
will be reported in the final analysis at study end). A full ≥61 years 2506 (12·7%) 2498 (12·7%)
list of study endpoints, including endpoints not reported BMI, kg/m² 25·7 (23·0–29·0) 25·7 (23·0–29·0)
on in this study, with reasons for omission, is included in Comorbidities
the appendix (p 8). Hypertension 1173 (5·9%) 1160 (5·9%)
Obesity 881 (4·5%) 890 (4·5%)
Statistical analysis (BMI >30 kg/m²)
HERALD is an event-driven trial, and sample size Diabetes 301 (1·5%) 312 (1·6%)
and power considerations were based on the primary Chronic 103 (0·5%) 103 (0·5%)
pulmonary
objective of showing the efficacy of CVnCoV in disease
preventing virologically confirmed cases of COVID-19 of Region or country*
any severity meeting the primary case definition.
Europe 5026/19 846 (25·3%) 5017/19 834 (25·3%)
Assuming a vaccine efficacy of 60%, with an overall
Belgium 1078/19 846 (5·4%) 1077/19 834 (5·4%)
two-sided α of 5%, we estimated that 160 participants
Germany 1405/19 846 (7·1%) 1406/19 834 (7·1%)
with COVID-19 of any severity, with a third of cases being
Netherlands 1082/19 846 (5·5%) 1078/19 834 (5·4%)
moderate to severe, were needed for the final analysis to
Spain 1461/19 846 (7·4%) 1456/19 834 (7·3%)
have a power of 90% to show a vaccine efficacy of more
Latin America 14 820/19 846 (74·7%) 14 817/19 834 (74·7%)
than 30% based on the lower bound of the CI for efficacy.
Argentina 3382/19 846 (17·0%) 3382/19 834 (17·1%)
Assuming a COVID-19 incidence of 0·15% per month in
Colombia 2178/19 846 (11·0%) 2178/19 834 (11·0%)
participants in the placebo group, an overall non-evaluable
Dominican 883/19 846 (4·4%) 884/19 834 (4·5%)
proportion of 20% (corresponding to participants Republic
excluded from the efficacy analysis set and those who
Mexico 3148/19 846 (15·9%) 3145/19 834 (15·9%)
dropped out), and a vaccine efficacy of 60%, we estimated
Panama 1504/19 846 (7·6%) 1502/19 834 (7·6%)
that 36 500 participants (18 250 per group) enrolled over
Peru 3725/19 846 (18·8%) 3726/19 834 (18·8%)
approximately 3 months would accrue 160 COVID-19
Serology status at baseline†
cases of any severity at approximately 9 months after the
Seronegative 17 093 (86·4%) 16 974 (86·0%)
first vaccination.
Seropositive 2311 (11·7%) 2404 (12·2%)
During case accrual, before the second interim analysis
Unknown 379 (1·9%) 368 (1·9%)
was done, we observed that the actual proportion of
Serology status at day 43†‡
participants with moderate-to-severe COVID-19 was
Seronegative 14 345 (72·5%) 12 951 (65·6%)
approximately 20%, which was lower than the expected 30%.
Seropositive 2220 (11·2%) 2257 (11·4%)
The protocol was amended to allow accrual of more cases
Unknown 3218 (16·3%) 4538 (23·0%)
to obtain the planned sample size (about 53 participants
with moderate-to-severe COVID-19) needed for the key Data are n (%), median (IQR), or n/N (%). The phase 2b–3 safety analysis set
comprises all participants who received at least one dose of CVnCoV or placebo,
secondary endpoint of measuring vaccine efficacy against
who are analysed in the group of the treatment dose received. BMI=body-mass
moderate-to-severe COVID-19. index. *Region and country data were evaluated in the population who were
Vaccine efficacy against symptomatic disease was randomly assigned. †Serology status was based on retrospective assessment
analysed in the primary efficacy analysis set, which using anti-SARS-CoV-2 nucleocapsid protein antibody concentrations. ‡Day 43
was the first day of COVID-19 case collection, 14 days after the second dose;
comprised all participants in the phase 2b and phase 3 serology status was not available for all participants at the time of database lock.
parts of the trial who received both doses of either
CVnCoV or placebo according to their treatment Table 1: Baseline and day 43 characteristics in the phase 2b–3 safety
analysis set
allocation, had not developed virologically confirmed
COVID-19 before day 43 (15 days after the second dose),
and were SARS-CoV-2-naive at baseline and day 43. the primary analysis, the hypothesis was tested with the
Vaccine efficacy was defined as 1 minus the ratio of exact test for binomial proportions. The trial was
the attack rate in participants receiving CVnCoV to considered successful if the lower limit of the exact
participants receiving placebo, multiplied by 100. In each two-sided Clopper-Pearson 95% CI (subject to adjustment
group, the attack rate was defined as the number of for multiple testing according to the cumulative
participants presenting with virologically confirmed O’Brien-Fleming type error spending function, giving an
COVID-19 divided by the total follow-up time. For actual CI of 95·826%) of the primary efficacy endpoint
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 5
Articles
which comprised all participants in the phase 2b and
CVnCoV Placebo Vaccine efficacy
phase 3 parts of the trial who received at least one dose
(95% CI)
of CVnCoV or placebo, according to the actual
n/N Person- n/N Person-
dose received. All analyses were done by use of
years years
SAS, version 9.4. For the primary outcome, a p value of
COVID-19 of any severity
less than 0·02087 was considered significant. This trial
Overall 83/12 851 1735·29 145/12 211 1569·87 48·2% (31·0–61·4)*
is registered at ClinicalTrials.gov, NCT04652102, and
18–60 years 71/11 532 1591·47 136/11 031 1449·23 52·5% (36·2–64·8) EudraCT, 2020–003998–22.
≥61 years 12/1319 143·82 9/1180 120·64 ··†
COVID-19 of any severity by region‡ Role of the funding source
Europe 21/4091 684·22 33/3919 604·83 43·7% (–0·2 to 69·1) CureVac was responsible for trial design and conduct,
Latin America 62/8760 1051·07 112/8292 965·03 49·2% (30·1–63·3) data analysis, data interpretation, and writing of the
COVID-19 of any severity by strain§ report. The German Federal Ministry of Education and
Alpha variant 20/11 532 1591·47 42/11 031 1449·23 55·1% (23·5–73·6) Research had no role in study design, data collection,
(B.1.1.7/501Y.V2)
data analysis, data interpretation, or writing of the report.
Gamma variant 9/11 532 1591·47 26/11 031 1449·23 67·1% (29·8–84·6)
(P.1/501Y.V3)
Lambda variant (C.37) 13/11 532 1591·47 26/11 031 1449·23 52·8% (8·2–75·8)
Results
HERALD is an ongoing clinical trial and the cutoff date
Mu variant (B.1.621) 11/11 532 1591·47 17/11 031 1449·23 ··†
for this analysis was June 18, 2021. Between Dec 11, 2020,
Other 7/11 532 1591·47 13/11 031 1449·23 ··†
and April 12, 2021, 3999 participants were enrolled and
Moderate-to-severe COVID-19
randomly assigned in the phase 2b trial (appendix p 11),
Overall 12/12 851 1735·29 37/12 211 1569·87 70·7% (42·5–86·1)
of whom 3994 were vaccinated with at least one dose
18–60 years 9/11 532 1591·47 36/11 031 1449·23 77·2% (51·8–90·4)
(2007 received CVnCoV; 1987 received placebo).
≥61 years 3/1319 143·82 1/1180 120·64 ··†
Altogether, 39 680 participants were enrolled and
Severe COVID-19
randomly assigned in the phase 2b and phase 3 parts of
Overall 4/12 851 1735·29 10/12 211 1569·87 ··†
the trial, of whom 39 529 (99·6%) received at least
18–60 years 2/11 532 1591·47 9/11 031 1449·23 ··† one dose of CVnCoV (n=19 783) or placebo (n=19 746;
≥61 years 2/1319 143·82 1/1180 120·64 ··† figure 1). 25 participants who were randomly assigned to
*For COVID-19 of any severity, the 95·826% CI is provided (due to adjustment for multiplicity across interim analyses). placebo received at least one dose of CVnCoV, and
†Not reported; the number of cases was too low to be statistically meaningful. ‡Vaccine efficacy by region was six participants who were randomly assigned to CVnCoV
evaluated post-hoc. §Efficacy against strains was evaluated in adjudicated and sequenced cases in participants aged
18–60 years; other strains includes B.1 lineage SARS-CoV-2. received two doses of placebo. Any participant who
received at least one dose of CVnCoV was considered as
Table 2: Efficacy of CVnCoV against virologically confirmed COVID-19 occurring 15 days or more after the being in the CVnCoV group for the safety analyses. Both
second dose in the primary efficacy analysis set
groups had similar demographic characteristics (table 1).
Before the final efficacy analysis, 14 410 (36·5%) of
(COVID-19 cases of any severity) was more than 30%. 39 529 vaccinated participants requested to be unmasked
Success for key secondary endpoints was defined as the (6715 [33·9%] of 19 783 in the CVnCoV group;
lower limit of the exact two-sided 95% CI being more 7695 [39·0%] of 19 746 in the placebo group), as allowed
than 20% for moderate-to-severe disease, and more per protocol when a SARS-CoV-2 vaccine became
than 10% for severe disease. Kaplan-Meier curves and available. 3494 (69·8%) of 5004 participants aged 61 years
associated log-rank tests were done in a key prespecified or older were unmasked, compared with 10 913 (31·6%)
sensitivity analysis to evaluate time to first occurrence of 34 525 participants aged 18–60 years. These unmasked
of virologically confirmed COVID-19. Post-hoc, we participants were censored in the efficacy analysis at the
evaluated vaccine efficacy by region. time of unmasking. Reasons for exclusion from the
Solicited adverse events were evaluated in the phase 2b primary efficacy analysis set have not yet been analysed
reactogenicity analysis set, which comprised all par per treatment group, but the most frequent reasons were
ticipants in the phase 2b part of the trial who received at positive or missing serostatus result at baseline or day 43,
least one dose of CVnCoV or placebo according to unmasked within 15 days after the second dose, did not
treatment received and for whom at least one diary receive two doses of randomised treatment, or developed
entry reporting the presence or absence of a solicited COVID-19 disease, discontinued the trial, or received a
adverse event was available. Unsolicited adverse events licenced COVID-19 vaccine within 15 days after the
were evaluated in the phase 2b safety analysis set, which second dose.
comprised all participants in the phase 2b part of the The primary efficacy analysis included 12 851 participants
trial who received at least one dose of CVnCoV or in the CVnCoV group and 12 211 in the placebo group.
placebo according to treatment received. Serious The mean observation period, starting 15 days after
adverse events and adverse events of special interest administration of the second dose, was 48·2 days
were assessed in the phase 2b/3 safety analysis set, (SE 0·2). Of the 228 adjudicated COVID-19 cases of any
6 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
Articles
severity caused by any strain, 83 occurred in the CVnCoV
A
group after a total follow-up of 1735·29 person-years and
100·000
145 occurred in the placebo group after a total follow-up of
1569·87 person-years, resulting in a vaccine efficacy 0·020 CVnCoV
Proportion with virologically confirmed
Placebo
against symptomatic disease of 48·2% (95·826% CI
COVID-19 of any severity (%)
31·0–61·4; p=0·016) in the overall study population 0·015
(table 2). 179 (79%) of the 228 COVID-19 cases were mild.
In participants aged 18–60 years, 71 adjudicated cases 0·010
of COVID-19 occurred in the CVnCoV group after
1591·47 person-years of follow-up and 136 occurred in the
0·005
placebo group after 1449·23 person-years of follow-up
(vaccine efficacy 52·5%, 95% CI 36·2–64·8). There
were too few participants aged 61 years or older with 0
0 30 60 90
virologically confirmed COVID-19 to evaluate vaccine Number at risk
efficacy in this age group (table 2). We show the (number censored); cases
cumulative incidence of symptomatic COVID-19 starting CVnCoV 12 851 (0); 0 10 404 (1389); 58 3888 (8881); 82 816 (11 952); 83
Placebo 12 211 (0); 0 9494 (2609); 108 3333 (8734); 144 560 (11 506); 145
on day 43 in the primary efficacy analysis set for all
participants (figure 2A) and those aged 18–60 years B
(figure 2B). 100·000
Overall, 49 participants (12 in the CVnCoV group and
0·020
37 in the placebo group) developed moderate-to-severe
Proportion with virologically confirmed
COVID-19, against which vaccine efficacy was 70·7%
COVID-19 of any severity (%)
0·015
(table 2). Of these, 45 participants were aged 18–60 years
(nine in the CVnCoV group and 36 in the placebo group),
for whom vaccine efficacy was 77·2% (table 2). The 0·010
number of cases of moderate-to-severe COVID-19 in
participants aged 61 years or older and the number 0·005
of participants with severe COVID-19 overall were
insufficient to meaningfully evaluate vaccine efficacy
0
(table 2). 0 30 60 90
Vaccine efficacy was similar between Europe and Number at risk
Days
Latin America in post-hoc analyses (table 2). Sequence (number censored); cases
data were available for 184 of 207 adjudicated cases in CVnCoV 11 532 (0); 0 9630 (1854); 48 3602 (7860); 70 750 (10 711); 71
Placebo 11 031 (0); 0 8837 (2092); 102 3120 (7776); 135 522 (10 373); 136
people aged 18–60 years. Seven (3%; two in the CVnCoV
group and five in the placebo group) of these cases in Figure 2: Kaplan-Meier cumulative incidence of virologically confirmed COVID-19 of any severity in the
the overall population were wild-type, defined as primary efficacy analysis set
(A) Overall study population. (B) Participants aged 18–60 years. On the graphs, day 0 corresponds to day 43 of the
WT/D614G lineages A.1/B.1 without the B.1.1.7 (alpha), study, which is 15 days after administration of the second dose. Data are not shown for participants aged 61 years
B.1.351 (beta), and B. 1.429 (epsilon) variants of concern. A or older as there were too few events to be statistically meaningful. Participants were censored if they were
full list of sequenced variants is presented in the unmasked, received an authorised COVID-19 vaccine, or discontinued participation in the trial for any other
appendix (p 9). 102 (50%) of 204 cases of COVID-19 were reason; censoring started on the day the event occurred. Log-rank tests evaluating group differences were
significant (p<0·0001) in the overall study population and the 18–60 years age group.
caused by variants of concern, and 23 (35%) were caused
by variants of interest. The remaining cases were caused
by wild type (seven [3%]) and various variants listed in the At least one solicited local or systemic adverse event was
appendix, p 8 (23 [11%]).14 In Europe, 45 (92%) of 49 cases reported by 1933 (96·5%) of 2003 participants in the
were caused by the alpha variant (the remaining four CVnCoV group, with 542 (27·1%) reporting grade 3
cases were caused by the gamma variant [P.1; two], by the events, and by 1344 (67·9%) of 1978 participants in the
delta variant [B.1.617.2; one], and by an unidentified variant placebo group, with 61 (3·1%) reporting grade 3 events
at the time [one]). In Latin America, 20 (13%) of 155 cases (table 3). Local reactions were more common in
were caused by the alpha variant, 34 (22%) were caused participants receiving CVnCoV than in those receiving
by the gamma variant, 43 (28%) were caused by the placebo (table 3; figure 3A, B). The most frequently
lambda variant of interest (C.37), and 29 (19%) were reported local reaction after any dose in the CVnCoV
caused by the Mu variant of interest (B.1.621). The group was injection-site pain (83·6%, 1678 of 2007), with
remaining cases were caused by alpha (20 [13%]), B.1.526 22 grade 3 reactions. Local reactions were transient, with a
(iota; one [1%]), wild-type (seven [5%]), P.2 (zeta; one [1%]), median duration of 2 days for pain and 1 day for redness,
and other (20 [13%]). Vaccine efficacies against the alpha, swelling, and itching in participants receiving CVnCoV
gamma, and lambda variants in people aged 18–60 years (appendix p 10). The median duration of all grade 3 local
were similar to the overall efficacy (table 2). reactions was 1 day for all reactions (appendix p 8).
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 7
Articles
were slightly higher in the CVnCoV group than in the
CVnCoV Placebo
placebo group (table 3). The most frequently reported
Any solicited adverse event* unsolicited adverse events in the CVnCoV group were
Overall 1933/2003 (96·5%) 1344/1978 (67·9%) headache (210 [10·4%] of 2007; 42 [2·1%] considered
Grade 3 542/2003 (27·1%) 61/1978 (3·1%) vaccine-related) and nasal congestion (127 [6·3%];
Local 1699/2003 (84·8%) 477/1978 (24·1%) 28 [1·4%] considered vaccine-related).
Grade 3 25/2003 (1·2%) 1/1978 (<0·1%) 176 serious adverse events were reported by 148 (0·4%)
Systemic 1881/2003 (93·9%) 1255/1978 (63·4%) of 39 529 participants in the phase 2b–3 safety analysis set
Grade 3 536/2003 (26·8%) 60/1978 (3·0%) (table 3). 100 serious adverse events occurred in 82 (0·4%)
Any unsolicited adverse event* of 19 783 participants in the CVnCoV group and 76 serious
Overall 1010/2007 (50·3%) 898/1987 (45·2%) adverse events occurred in 66 (0·3%) of 19 746 participants
Grade 3 45/2007 (2·2%) 38/1987 (1·9%) in the placebo group. Eight serious adverse events in five
Considered 510/2007 (25·4%) 268/1987 (13·5%) CVnCoV recipients (acute myocardial infarction, atrial
vaccination-related fibrillation, and cardiac arrest [n=1]; supraventricular
Any serious adverse event† extrasystoles and ventricular tachycardia [n=1], appendi
Overall 82/19 783 (0·4%); 100 66/19 746 (0·3%); 76 citis [n=1], cellulitis [n=1], and seizure [n=1]) and two serious
Considered 5/19 783 (<0·1%); 8 2/19 746 (<0·1%); 2 adverse events in two placebo recipients (hypersensitivity
vaccination-related [n=1] and deep vein thrombosis [n=1]) were considered
Any adverse event of special interest† vaccination-related by study investigators. Fatal adverse
Overall 38/19 783 (0·2%); 44 31/19 746 (0·2%); 35 events were reported for eight participants in the CVnCoV
Considered 14/19 783 (0·1%); 18 5/19 746 (<0·1%); 6 group and for six participants in the placebo group, none
vaccination-related
of which were considered related to vaccination (table 3).
Any adverse event with fatal outcome†
Adverse events of special interest were reported for
Overall 8/19 783 (<0·1%) 6/19 746 (<0·1%)
38 participants (0·2%) in the CVnCoV group and
Considered 0 0
31 participants (0·2%) in the placebo group. Adverse
vaccination-related
events of special interest considered to be related to the
Data are n/N (%) or n/N (%); number of events. Serious adverse events are
trial vaccine were reported for 14 participants (<0·1%) in
reported from immediately after the second dose to the date of data cutoff
(June 18, 2021). *Solicited and unsolicited adverse events were analysed in the the CVnCoV group and for five participants (<0·1%) in the
reactogenicity analysis set, which comprised participants in the phase 2b trial who placebo group. The primary safety outcomes for 1 year
received at least one dose of CVnCoV or placebo and and for whom at least one after the second dose are not provided to preserve study
diary entry reporting the presence or absence of a solicited adverse event was
available (phase 2b reactogenicity) and all participants who had received at least
blinding. Data for these outcomes up to 1 year will be
one dose of CVnCoV or placebo (phase 2b safety). In the phase 2b part of the reported in a future publication.
study, solicited local and systemic adverse events were reported in participant
diaries for 7 days following any dose and unsolicited adverse events were reported
in participant diaries for 28 days following any dose. †Serious adverse events and
Discussion
adverse events of special interest or with a fatal outcome were analysed in the The phase 2b/3 HERALD trial evaluating the CVnCoV
phase 2b–3 safety analysis set, which comprised all participants who received at vaccine candidate met the prespecified success criteria for
least one dose of CVnCoV or placebo; participants were analysed in the group efficacy against symptomatic COVID-19 of any severity
corresponding to the dose they actually received.
(lower limit of the 95% CI >30%) and for efficacy against
Table 3: Adverse events moderate-to-severe COVID-19 (lower limit of the 95% CI
>20%), as defined in the protocol. WHO guidelines
Solicited systemic reactions, and grade 3 solicited systemic recommend a lower bound of at least 30% and a vaccine
reactions, were also more common in participants in the efficacy of at least 50%.15 Vaccine efficacy against
CVnCoV group than in those in the placebo group (table 3; COVID-19 of any severity was 48·2% (95·826% CI
figure 3C, D). The most frequently reported solicited 31·0–61·4) in the overall primary efficacy analysis set of
systemic reactions after any dose in participants receiving SARS-CoV-2-naive participants, and 52·5% (95% CI
CVnCoV were fatigue (1603 [80·0%] of 2003) and 36·2–64·8) in those aged 18–60 years. Vaccine efficacy
headache (1541 [76·9%]). The median duration of systemic against moderate-to-severe COVID-19 was 70·7%
reactions was 2 days for headache, fatigue, and myalgia, (42·5–86·1) overall and 77·2% (51·8–90·4) in participants
and 1 day for fever, chills, arthralgia, nausea or vomiting, aged 18–60 years. There were too few participants aged
and diarrhoea in CVnCoV recipients (appendix p 10). The 61 years or older who developed COVID-19 to allow a
median duration of grade 3 systemic reactions was 1 day meaningful estimate of efficacy in this age group.
for all reactions (appendix p 10). No increase in solicited Although the prevalence of solicited and unsolicited
reactions was seen between the first and second CVnCoV adverse events was higher in CVnCoV recipients than in
doses (figure 3). placebo recipients, these events were transient and mostly
The proportions of participants reporting unsolicited mild-to-moderate (grade 1–2). The proportion of CVnCoV
adverse events and grade 3 unsolicited adverse events recipients reporting solicited local and systemic adverse
occurring during the 28 days following any vaccination events in the 7 days following any dose was similar to that
8 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
Articles
A Dose 1 B Dose 2
Placebo
Pain
CVnCoV
Placebo
Solicited systemic adverse events
Redness
CVnCoV
Placebo
Swelling
CVnCoV
Placebo
Itching
Grade 1–2 CVnCoV
CVnCoV Grade 1–2 placebo
Grade 3
C Dose 1 D Dose 2
Placebo
Fever
CVnCoV
Headache
Placebo
CVnCoV
Fatigue
Placebo
CVnCoV
Solicited systemic adverse events
Placebo
Chills
CVnCoV
Nausea Arthralgia Myalgia
Placebo
CVnCoV
Placebo
CVnCoV
or vomiting
Placebo
CVnCoV
Diarrhoea
Placebo
CVnCoV
0 10 20 30 40 50 60 70 80 90 100 0 10 20 30 40 50 60 70 80 90 100
Proportion of participants (%) Proportion of participants (%)
Figure 3: Solicited local and systemic adverse events in the phase 2b reactogenicity analysis set
Solicited local adverse events occurring within 7 days of the first dose (A) and the second dose (B), and solicited systemic adverse events occurring within 7 days of the
first dose (C) and the second dose (D).
seen in other mRNA vaccine phase 3 trials.7,8 No increase although the short follow-up duration needs to be
in solicited reactions was seen between the first and second considered when interpreting these findings. The safety
CVnCoV doses. Serious adverse events and adverse events of the CVnCoV vaccine candidate will continue to be
of special interest were uncommon and similar in monitored for the duration of the trial, and findings will
frequency between the CVnCoV and placebo groups, be presented in a future publication. Taken together with
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 9
Articles
the safety data from phase 1 trials with CVnCoV and with analysis set and 10·0% (2499 of 25 062) of participants in
the CV7202 rabies mRNA vaccine,11,16 the findings observed the primary efficacy analysis set were aged 61 years or
in this trial provide further support for the safety of the older. In addition, 69·8% of participants aged 61 years or
RNActive mRNA vaccine platform.17 older in the primary efficacy analysis set were unmasked
HERALD was conducted in an unprecedented evolving compared with 31·6% of those aged 18–60 years.
landscape that reflects the changing reality of the global This unblinding resulted in markedly fewer analysable
COVID-19 pandemic, with an increasing number of participants aged 61 years or older in our study than in
SARS-CoV-2 variants adding additional challenges to most other phase 3 efficacy trials assessing COVID-19
the assessment of COVID-19 vaccine candidates. The vaccines.7,8,20,23,25 The low recruitment, combined with the
mRNA component of the CVnCoV vaccine candidate large number of older participants who were unmasked
encodes the SARS-CoV-2 spike protein, like the and therefore contributed less follow-up time to the
two mRNA vaccines (BNT162b2 and mRNA-1273) that efficacy analyses, limited the interpretability of our
have been approved as of August, 2021. However, only 3% findings in this age group and affected the overall study
of adjudicated and sequenced cases of COVID-19 in results.
HERALD were identified as resulting from B.1 lineage The broad case definition and the twice weekly reminders
SARS-CoV-2. About 50% of cases of COVID-19 in our to participants to report any potential COVID-19 symptoms
trial were caused by variants of concern, 35% were in HERALD meant that symptoms that probably would
caused by variants of interest, as classified by WHO in not have triggered RT-PCR confirmation in other trials of
September, 2021, and about 3% were caused by wild-type, SARS-CoV-2 vaccines might have resulted in confirmation
with the remaining 11% caused by other variants.14 of mild COVID-19 in HERALD, as evidenced by the fact
Although we were only able to evaluate vaccine efficacy that almost 80% of cases were mild. Most vaccines,
against these variants in participants aged 18–60 years, including CVnCoV, have shown increased efficacy against
the results indicate that the vaccine had similar efficacies COVID-19 with increasing disease severity.7,8,23,25 The
against alpha, gamma, and lambda variants. Many newly clinical implications of CVnCoV’s 70·7% efficacy against
emerged strains have shown increased transmissibility,18 moderate-to-severe COVID-19, nearly all cases of which
and differences in neutralising antibody activity against were caused by variants of concern or variants of interest,
these strains might alter vaccine efficacy.19 These suggest a high potential for a positive impact on public
concerns are supported by results from other phase 3 health. Access to vaccines protecting against moderate-to-
efficacy trials, with SARS-CoV-2 variant-dependent severe disease, and thus preventing disruption to the
differences in efficacy reported for the ChAdOx1 nCoV-19 normal functioning of hospitals and intensive care units,
(Oxford-AstraZeneca),20–22 NVX-CoV2373 (Novavax),23,24 is essential to prevent non-COVID-19-associated morbidity
and Ad26.COV2.S (Janssen) SARS-CoV-2 vaccines.25 The and mortality.29–31
point estimates for real-world mRNA vaccine effectiveness, CVnCoV contains 12 μg of mRNA, considerably less
in settings with increasing diversity of variants, are lower than BNT162b2 (30 μg) and mRNA-1273 (100 μg) contain.
than the point estimates for efficacy as reported in We cannot dismiss the possibility that this dose was
clinical trials.26–28 In this context, the comparison of insufficient to elicit a protective immune response.
vaccine efficacy against different SARS-CoV-2 variants However, in a phase 1 dose-escalation study of participants
and between Europe and Latin America, although not aged 18–60 years, two 12 μg doses of CVnCoV induced
prespecified in the protocol, is important from a public antibodies against the SARS-CoV-2 spike protein
health perspective. Broad geographical representation and its receptor binding domain and anti-SARS-CoV-2
should therefore be considered when designing future neutralising titres that were similar to those seen in
studies evaluating the efficacy of SARS-CoV-2 vaccines convalescent serum samples from patients who had had
and vaccine efficacy against emerging variants. COVID-19.11 However, in view of the changing
HERALD was initiated when the first SARS-CoV-2 environment, including the emergence of SARS-CoV-2
vaccines were authorised for emergency use. As national variants, and taking into account timelines for further
COVID-19 vaccination programmes prioritised the development, the decision had been made to cease
vaccination of older adults, recruiting non-vaccinated activities on the CVnCoV candidate, and to focus efforts
participants aged 61 years or older was difficult, and this on the promising and rapidly progressing development of
limitation might have contributed to the proportion of the next generation vaccine candidates. One of these, the
the study population aged 61 years or older being less CV2CoV candidate, has already been shown to induce
than the non-binding target enrolment of 20–25%. In high humoral and cellular immune responses in non-
addition, per protocol, participants eligible for an human primate studies.32
authorised vaccine could request unmasking and In conclusion, the two-dose regimen of CVnCoV had
subsequent vaccination with an available vaccine, an acceptable safety profile and was efficacious in the
and this allowance resulted in further censoring of prevention of symptomatic COVID-19 in adults. In
participants in the efficacy analyses. Only 12·7% (5004 of addition, we observed vaccine efficacy against newly
39 529) of the participants in the phase 2b–3 safety emerged variants, including variants of concern.
10 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
Articles
Contributors but are nonetheless recognised for their tireless work, which is still
PGK, AK, IL-R, PM, OS-K, TV, and LO conceived the HERALD trial; ongoing. Special thanks go to the members of the DMSB, chaired by
PGK is the coordinating investigator and LO is study lead. HJ is the Fred Zepp.
qualified physician and co-chair of the DSMB. PGK, RC, EJLDB, MAGG,
References
AK, IL-R, PM, MFM-R, OS-K, TV, and LO contributed to the trial design 1 WHO. WHO coronavirus (COVID-19) dashboard. 2021.
and protocol. PGK, HJ, PM, and TV participated in the data curation and https://covid19.who.int/ (accessed Aug 12, 2021).
had full access to and verified all study data. PGK, AK, PM, OS-K, TV, 2 WHO. WHO Director-General’s opening remarks at the media
and LO did the statistical analyses. PGK, RAAG, EA-A, GJAM, MB, RC, briefing on COVID-19—11 March 2020. March 11, 2020.
RC GC, EJLDB, LE, JJG, CAGL, LG, MAGG, NG, MPG, ADH, CFL, CL, https://www.who.int/director-general/speeches/detail/who-director-
IL-R, MFM-R, TJO, CAP, MJRF, LMRM, VVRH, XS-L, MS, ASG, IV, and general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-
MV are study site principal investigators. PGK, PM, OS-K, and LO were march-2020 (accessed Sept 22, 2021).
in the core writing group responsible for preparation of the manuscript 3 Gavi, the Vaccine Alliance. The COVID-19 vaccine race—weekly
and received support from a medical writer. Manuscript drafts were update. Sept 19, 2021. https://www.gavi.org/vaccineswork/covid-19-
reviewed by all authors, and the content of the submitted version was vaccine-race (accessed Sept 22, 2021).
approved by all authors before submission. All authors had final 4 Huang Q, Yan J. SARS-CoV-2 virus: vaccines in development.
responsibility for the decision to submit for publication. Because the Fundamental Res 2021; 1: 131–38.
study is ongoing, authors could not be given access to the whole dataset 5 Pardi N, Hogan MJ, Porter FW, Weissman D. mRNA vaccines—a
analysed in this Article, but they will be given full access when the study new era in vaccinology. Nat Rev Drug Discov 2018; 17: 261–79.
is terminated. 6 Jackson NAC, Kester KE, Casimiro D, Gurunathan S, DeRosa F.
The promise of mRNA vaccines: a biotech and industrial
Declaration of interests perspective. NPJ Vaccines 2020; 5: 11.
MB declares institutional funding from CureVac during the conduct of 7 Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the
this study, institutional funding from Janssen Vaccines, BNT162b2 mRNA COVID-19 vaccine. N Engl J Med 2020;
Molecular Partners, and Merck outside the submitted work, and 383: 2603–15.
consulting fees from Janssen Vaccines outside the submitted work. 8 Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the
EJLDB, MFM-R, TJO, and XS-L declare institutional funding from mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021; 384: 403–16.
CureVac during the conduct of this study. LE and LG declare 9 Rauch S, Roth N, Schwendt K, Fotin-Mleczek M, Mueller SO,
institutional funding from CureVac during the conduct of this study and Petsch B. mRNA-based SARS-CoV-2 vaccine candidate CVnCoV
outside the submitted work. CFL declares institutional funding from induces high levels of virus-neutralising antibodies and mediates
CureVac during the conduct of this study and outside the submitted protection in rodents. NPJ Vaccines 2021; 6: 57.
work and is a member of the WHO Covid-19 Vaccine Effectiveness 10 Rauch S, Gooch K, Hall Y, et al. mRNA vaccine CVnCoV protects
Working Group and the WHO Product Development for Vaccines non-human primates from SARS-CoV-2 challenge infection. bioRxiv
Advisory Committee. CL declares institutional funding from CureVac 2020; published online Dec 23. https://doi.
during the conduct of this study and is a member of the German Society org/10.1101/2020.12.23.424138 (preprint).
of Infection board. IL-R declares institutional funding from CureVac 11 Kremsner PG, Mann P, Kroidl A, et al. Safety and immunogenicity
during the conduct of this study and institutional funding from of an mRNA-lipid nanoparticle vaccine candidate against
Johnson & Johnson and OSE Immunotherapeutics outside the SARS-CoV-2: a phase 1 randomized clinical trial.
submitted work. PGK declares institutional funding from CureVac Wien Klin Wochenschr 2021; 133: 931–41.
during the conduct of this study and is a member of the scientific 12 US Department of Health and Human Services. US Food and Drug
advisory board for the HERALD clinical trial. VVRH declares Administration. Development and licensure of vaccines to prevent
COVID-19. Guidance for industry. June, 2020. https://www.fda.gov/
institutional funding from CureVac during the conduct of this study and
regulatory-information/search-fda-guidance-documents/development-
speakers fees from Gilead outside the submitted work. HJ declares
and-licensure-vaccines-prevent-covid-19 (accessed July 27, 2021).
consultant fees from CureVac, is the qualified physician for the
13 US Department of Health and Human Services. US Food and Drug
HERALD clinical trial, and is co-chair of the DSMB for the Administration. COVID-19: developing drugs and biological
HERALD clinical trial. AK and PM are employed by CureVac and hold products for treatment or prevention. Guidance for industry.
stock options. OS-K declares consultant fees from CureVac during the May, 2020 https://www.fda.gov/regulatory-information/search-fda-
conduct of this study and is a member of the DSMB for a CVnCoV guidance-documents/covid-19-developing-drugs-and-biological-
phase 1 trial. TV declares consultant fees from CureVac during the products-treatment-or-prevention (accessed July 27, 2021).
conduct of this study, and consultant fees from CureVac, AstraZeneca, 14 WHO. Tracking SARS-CoV-2 variants. 2021. https://www.who.int/
Pfizer, Johnson & Johnson, and Moderna outside the submitted work. en/activities/tracking-SARS-CoV-2-variants/ (accessed July 27, 2021).
LO is employed by CureVac and holds stock options and is the holder of 15 WHO. Considerations for evaluation of COVID19 vaccines.
a pending patent. All other authors declare no competing interests. November, 2020. https://cdn.who.int/media/docs/default-source/
in-vitro-diagnostics/covid19/considerations-who-evaluation-of-covid-
Data sharing vaccine_v25_11_2020.pdf (accessed Oct 1, 2021).
Anonymised participant data will be made available when the trial is
16 Aldrich C, Leroux-Roels I, Huang KB, et al. Proof-of-concept of a low-
complete, on requests directed to the corresponding author. Proposals dose unmodified mRNA-based rabies vaccine formulated with lipid
will be reviewed and approved by the sponsor, investigator, and nanoparticles in human volunteers: a phase 1 trial. Vaccine 2021;
collaborators on the basis of scientific merit. After approval of a 39: 1310–18.
proposal, data can only be shared through a secure online platform after 17 Rauch S, Lutz J, Kowalczyk A, Schlake T, Heidenreich R.
a data access agreement is signed. All data will be made available for a RNActive® technology: generation and testing of stable and
minimum of 5 years from the end of the trial. immunogenic mRNA vaccines. Methods Mol Biol 2017;
1499: 89–107.
Acknowledgments
This study was funded by the German Federal Ministry of Education and 18 Hossain MK, Hassanzadeganroudsari M, Apostolopoulos V.
The emergence of new strains of SARS-CoV-2. What does it mean
Research (grant 01KI20703) and CureVac. Draft versions of this
for COVID-19 vaccines? Expert Rev Vaccines 2021; 20: 635–38.
manuscript were reviewed by Giulia Povellato and Robert Tensen
19 Garcia-Beltran WF, Lam EC, St Denis K, et al. Multiple SARS-CoV-2
(Medical Affairs Department, CureVac, Frankfurt, Germany). Medical
variants escape neutralization by vaccine-induced humoral
writing services were provided by Jarno Jansen and Margaret Haugh, immunity. Cell 2021; 184: 2372–83.e9.
who also provided editorial support, both funded by CureVac. We thank
20 Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the
all study participants for their contribution to HERALD. We also thank ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2:
all staff at the clinical study centres, the contract research organisations, an interim analysis of four randomised controlled trials in Brazil,
the laboratories, and in CureVac, who are too numerous to be named South Africa, and the UK. Lancet 2021; 397: 99–111.
www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0 11
Articles
21 Emary KRW, Golubchik T, Aley PK, et al. Efficacy of ChAdOx1 28 Nasreen S, He S, Chung H, et al. Effectiveness of COVID-19
nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern vaccines against variants of concern, Canada. medRxiv 2021;
202012/01 (B.1.1.7): an exploratory analysis of a randomised published online July 3. https://doi.org/10.1101/2021.06.28.21259420
controlled trial. Lancet 2021; 397: 1351–62. (preprint).
22 Madhi SA, Baillie V, Cutland CL, et al. Efficacy of the ChAdOx1 29 Berg GM, Wyse RJ, Morse JL, et al. Decreased adult trauma
nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med admission volumes and changing injury patterns during the
2021; 384: 1885–98. COVID-19 pandemic at 85 trauma centers in a multistate healthcare
23 Heath PT, Galiza EP, Baxter DN, et al. Safety and efficacy of system. Trauma Surg Acute Care Open 2021; 6: e000642.
NVX-CoV2373 Covid-19 vaccine. N Engl J Med 2021; 385: 1172–83. 30 Woolf SH, Chapman DA, Sabo RT, Weinberger DM, Hill L,
24 Shinde V, Bhikha S, Hoosain Z, et al. Efficacy of NVX-CoV2373 Taylor DDH. Excess deaths from COVID-19 and other causes,
Covid-19 vaccine against the B.1.351 variant. N Engl J Med 2021; March-July 2020. JAMA 2020; 324: 1562–64.
384: 1899–909. 31 Dopfer C, Wetzke M, Zychlinsky Scharff A, et al. COVID-19 related
25 Sadoff J, Gray G, Vandebosch A, et al. Safety and efficacy of reduction in pediatric emergency healthcare utilization—a
single-dose Ad26.COV2.S vaccine against Covid-19. N Engl J Med concerning trend. BMC Pediatr 2020; 20: 427.
2021; 384: 2187–201. 32 Gebre MS, Rauch S, Roth N, et al. Optimization of non-coding
26 Kustin T, Harel N, Finkel U, et al. Evidence for increased regions for a non-modified mRNA COVID-19 vaccine. Nature 2021;
breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2- published online Nov 18. doi:10.1038/s41586-021-04231-6.
mRNA-vaccinated individuals. Nat Med 2021; 27: 1379–84.
27 Puranik A, Lenehan PJ, Silvert E, et al. Comparison of two highly-
effective mRNA vaccines for COVID-19 during periods of alpha and
delta variant prevalence. medRxiv 2021; published online Aug 21.
https://doi.org/10.1101/2021.08.06.21261707 (preprint).
12 www.thelancet.com/infection Published online November 23, 2021 https://doi.org/10.1016/S1473-3099(21)00677-0
You might also like
- Architecture in The Post Pandemic WorldDocument3 pagesArchitecture in The Post Pandemic WorldFashionable JewelleryNo ratings yet
- Cool Planning HandbookDocument154 pagesCool Planning Handbookrosecity08No ratings yet
- S9 Exam - 2017: HousingDocument30 pagesS9 Exam - 2017: HousingSandra BettyNo ratings yet
- MT Laurel - 0320Document24 pagesMT Laurel - 0320elauwitNo ratings yet
- Smart City Drad TDocument94 pagesSmart City Drad Tsayali pitaleNo ratings yet
- Central Bank Digital Currency Opportunities Challenges and DesignDocument57 pagesCentral Bank Digital Currency Opportunities Challenges and DesignLudovicoNo ratings yet
- Banking On Social MediaDocument7 pagesBanking On Social MediaSaurabh GaiakwadNo ratings yet
- Chapter 1 5 For HardboundDocument84 pagesChapter 1 5 For Hardbounddaniea smithNo ratings yet
- Current Trends in Civil & Structural EngineeringDocument2 pagesCurrent Trends in Civil & Structural EngineeringsrikantheraNo ratings yet
- 3D Ger AnalyzerDocument7 pages3D Ger AnalyzertomasmabotaNo ratings yet
- Policy Lab Series On Affordable Rental Housing - Summary of DiscussionsDocument55 pagesPolicy Lab Series On Affordable Rental Housing - Summary of DiscussionsAnkita Vinchoorkar100% (1)
- WEF Bridging Digital and Environmental Goals 2021-2Document27 pagesWEF Bridging Digital and Environmental Goals 2021-2EHS TRAINERNo ratings yet
- Affordable Housing ReportDocument48 pagesAffordable Housing ReportSeverus SnapeNo ratings yet
- WP Shaping ASEAN Future Readiness Report 2018Document29 pagesWP Shaping ASEAN Future Readiness Report 2018Loka GaneshanNo ratings yet
- Sipri - Trends in World Military Expenditure, 2017Document8 pagesSipri - Trends in World Military Expenditure, 2017nelson duringNo ratings yet
- LOW-INCOME HOUSING: ALTERNATIVE STRATEGIES FOR BUILDING CONSTRUCTION AND PROJECT CONTROL by JAVED SJLTANDocument221 pagesLOW-INCOME HOUSING: ALTERNATIVE STRATEGIES FOR BUILDING CONSTRUCTION AND PROJECT CONTROL by JAVED SJLTANAhmed UsmanNo ratings yet
- Asset Listing 2021Document123 pagesAsset Listing 2021Meksen MahiedineNo ratings yet
- Gianluca Mattarocci, Xenia Scimone - The New Era of Real Estate - An Analysis of Business Models in The Proptech Industry-Palgrave Pivot (2022)Document147 pagesGianluca Mattarocci, Xenia Scimone - The New Era of Real Estate - An Analysis of Business Models in The Proptech Industry-Palgrave Pivot (2022)scribdanonimoNo ratings yet
- General Awareness For RRB NTPC-UN and Other Important World OrganizationsDocument10 pagesGeneral Awareness For RRB NTPC-UN and Other Important World OrganizationsKaran SinghaniaNo ratings yet
- Wef The Future of Financial Infrastructure PDFDocument130 pagesWef The Future of Financial Infrastructure PDFerraticNo ratings yet
- Full Thesis (2021) - Ditmar PDFDocument133 pagesFull Thesis (2021) - Ditmar PDFKe'nan LundebaNo ratings yet
- Social Housing Provision in NigeriaDocument42 pagesSocial Housing Provision in NigeriaShem AyegbaNo ratings yet
- HLTH 101 Final Research Paper - Due 11 30Document7 pagesHLTH 101 Final Research Paper - Due 11 30api-625713699No ratings yet
- Real Estate March 2021Document33 pagesReal Estate March 2021Prem PrakashNo ratings yet
- Chapter One & Two (Land Use)Document38 pagesChapter One & Two (Land Use)mallamsamboNo ratings yet
- Central Bank Digital Currencies and Gold 1Document20 pagesCentral Bank Digital Currencies and Gold 1Júlio César CoelhoNo ratings yet
- Complete ProjectDocument54 pagesComplete ProjectAbhijit SahaNo ratings yet
- Current Affairs MCQs PDF - June 2022Document65 pagesCurrent Affairs MCQs PDF - June 2022ralteduhawmaNo ratings yet
- Southeast Ventures LLC Zoning Petition, WS/FC Planning Board. November 19, 2004.Document27 pagesSoutheast Ventures LLC Zoning Petition, WS/FC Planning Board. November 19, 2004.CP TewNo ratings yet
- Climate Proofing: A Risk-Based Approach To AdaptationDocument219 pagesClimate Proofing: A Risk-Based Approach To AdaptationAsian Development BankNo ratings yet
- Democracy Under Siege: Foreign Interference in A Digital EraDocument6 pagesDemocracy Under Siege: Foreign Interference in A Digital EraMartin S. PetlachNo ratings yet
- Strategies For Real Estate Development in TheDocument3 pagesStrategies For Real Estate Development in TheFernanda Rozendo SilvaNo ratings yet
- Real Estate and ConstructionsDocument23 pagesReal Estate and ConstructionsNiti KamdarNo ratings yet
- UN SG Roadmap Financing The SDGs July 2019Document67 pagesUN SG Roadmap Financing The SDGs July 2019Korean Institute of CriminologyNo ratings yet
- Jll-Capital Markets BrochureDocument12 pagesJll-Capital Markets BrochurechloeheNo ratings yet
- Rejuvenation in Rural Ireland in Response To The COVID-19 Induced Urban-To-Rural Migration PhenomenonDocument16 pagesRejuvenation in Rural Ireland in Response To The COVID-19 Induced Urban-To-Rural Migration PhenomenonIEREKPRESSNo ratings yet
- WEF Energy Transition 101 2020Document6 pagesWEF Energy Transition 101 2020Luis Pedrero OjedaNo ratings yet
- 2021 Update Assetmanagement Shadow BankingDocument62 pages2021 Update Assetmanagement Shadow Bankingzarin tasnimNo ratings yet
- Transportation and Logistics 2030 How Will Supply Chains Evolve in An Energy-Constrained Low Carbon WorldDocument64 pagesTransportation and Logistics 2030 How Will Supply Chains Evolve in An Energy-Constrained Low Carbon WorldstephlukNo ratings yet
- JLL Inland Port Marketing BrochureDocument4 pagesJLL Inland Port Marketing Brochuremutton moonswamiNo ratings yet
- Semiconductors: Lisa Bembenick - Naresh Bhaskar - Yi-Hsin Chen Yuan Chen - Teguh DjojoargonoDocument15 pagesSemiconductors: Lisa Bembenick - Naresh Bhaskar - Yi-Hsin Chen Yuan Chen - Teguh DjojoargonoJames Salig Jr.No ratings yet
- These Are Not Leases - You Own The Vehicle: 1500 Express Quad 4X4 Patriot Sport Hyundai SonataDocument48 pagesThese Are Not Leases - You Own The Vehicle: 1500 Express Quad 4X4 Patriot Sport Hyundai SonataThe WorldNo ratings yet
- Affordable Housing in ChinaDocument2 pagesAffordable Housing in ChinannafosNo ratings yet
- Drawdown Lift - Climate Poverty Connections Report - March 2022.2Document107 pagesDrawdown Lift - Climate Poverty Connections Report - March 2022.2Lenin Dender AguilarNo ratings yet
- Google Glass AbstractDocument3 pagesGoogle Glass AbstractibnurasheedaNo ratings yet
- SME Finance in CambodiaDocument15 pagesSME Finance in CambodiaADBI EventsNo ratings yet
- High Altitude Phisiology: Adiartha GriadhiDocument43 pagesHigh Altitude Phisiology: Adiartha GriadhilindaNo ratings yet
- Orchards Clinic Art Creates Dialgue On GBV KNDocument5 pagesOrchards Clinic Art Creates Dialgue On GBV KNJDANo ratings yet
- Death Wish ListDocument6 pagesDeath Wish ListphilippatstonNo ratings yet
- The Role of ICT in Mynmar DraftDocument10 pagesThe Role of ICT in Mynmar DraftYe Win HtutNo ratings yet
- Yojana February 2013 Direct Benefit TransferDocument57 pagesYojana February 2013 Direct Benefit TransferPriyatam BolisettyNo ratings yet
- Agriculture and Food Systems To 2050Document678 pagesAgriculture and Food Systems To 2050ERENo ratings yet
- Public Housing Delivery Strategies in NigeriaDocument9 pagesPublic Housing Delivery Strategies in NigeriaAbraham OwoseniNo ratings yet
- Chislett - 2021-Brexit Consequences For SpainDocument9 pagesChislett - 2021-Brexit Consequences For SpainIrene GarcíaNo ratings yet
- Investing in Clean Energy: How To Maximize Clean Energy Deployment From International Climate InvestmentsDocument58 pagesInvesting in Clean Energy: How To Maximize Clean Energy Deployment From International Climate InvestmentsCenter for American ProgressNo ratings yet
- Sustainability 13 11551 v2Document12 pagesSustainability 13 11551 v2Constantine KanelNo ratings yet
- Affordable Housing in Glendale BrochureDocument2 pagesAffordable Housing in Glendale BrochureGlendaleCDDNo ratings yet
- YB1944Document420 pagesYB1944Brendan Paul ValiantNo ratings yet
- PIIS014067362101429XDocument10 pagesPIIS014067362101429XRosamel FierroNo ratings yet
- PIIS0140673621015439Document3 pagesPIIS0140673621015439Rosamel FierroNo ratings yet
- Soros Foundation Offers ItsDocument1 pageSoros Foundation Offers ItsMerel GewoonNo ratings yet
- Soros Money Filters ThroughDocument1 pageSoros Money Filters ThroughMerel GewoonNo ratings yet
- Soros Foundation Is DefendedDocument1 pageSoros Foundation Is DefendedMerel GewoonNo ratings yet
- A Study of Stop-And-Search Practices in ParisDocument6 pagesA Study of Stop-And-Search Practices in ParisMerel GewoonNo ratings yet
- Operation Deep Freeze 50 Years of US Air Force Airlift in Antarctica 1956 2006Document284 pagesOperation Deep Freeze 50 Years of US Air Force Airlift in Antarctica 1956 2006Merel GewoonNo ratings yet
- Army Observers Report of Operation HighjumpDocument26 pagesArmy Observers Report of Operation HighjumpMerel GewoonNo ratings yet
- Population Resources Environment by The Ehrlichs (1972)Document536 pagesPopulation Resources Environment by The Ehrlichs (1972)matkan_lopussa6711100% (1)
- Joe Biden Was Chairman of This 'Dark Winter' Congressional ReportDocument108 pagesJoe Biden Was Chairman of This 'Dark Winter' Congressional ReportAll News PipelineNo ratings yet
- Ensuring The Public's Right To Know in The COVID-19 PandemicDocument17 pagesEnsuring The Public's Right To Know in The COVID-19 PandemicMerel GewoonNo ratings yet
- Fauci EmailsDocument3,234 pagesFauci EmailsCami Mondeaux89% (28)
- Reassurance at Every Step: Keeps Giving You More!Document33 pagesReassurance at Every Step: Keeps Giving You More!ansanthoshanNo ratings yet
- 5 OPD Waiting Time On Patient Satisfaction: April 2018Document6 pages5 OPD Waiting Time On Patient Satisfaction: April 2018Abdur Rashid KhanNo ratings yet
- Guillain-Barre Syndrome: Practice EssentialsDocument16 pagesGuillain-Barre Syndrome: Practice EssentialsUKMBasketNo ratings yet
- Inflammatory Bowel Disease (IBD)Document41 pagesInflammatory Bowel Disease (IBD)ririNo ratings yet
- Profile - D.SDocument2 pagesProfile - D.Sapi-3742748No ratings yet
- Neclex Questions Test 3Document16 pagesNeclex Questions Test 3Brittany Worrall100% (13)
- Skripsi Tanpa Bab Pembahasan PDFDocument112 pagesSkripsi Tanpa Bab Pembahasan PDFMaudiaazhara RaisaNo ratings yet
- Transient Tachypnea of NewbornDocument4 pagesTransient Tachypnea of NewbornloraineNo ratings yet
- Drug Study (Schizo)Document5 pagesDrug Study (Schizo)aliannaNo ratings yet
- Bauer 2019Document6 pagesBauer 2019RaffaharianggaraNo ratings yet
- Hyperemesis GravidarumDocument37 pagesHyperemesis GravidarumRamadhan GhaffarNo ratings yet
- PDFDocument11 pagesPDFNico IonaşcuNo ratings yet
- Clinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRDocument25 pagesClinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRChristian ErelNo ratings yet
- 2016 Revised Standards For Clinical Dental Hygiene PracticeDocument16 pages2016 Revised Standards For Clinical Dental Hygiene PracticeElvira PurnamasariNo ratings yet
- Komplikasi Dalam Kehamilan: Dr. Dian Ika Putri Syafaruddin, Spog Smf. Obgyn Rsud Soehadi Prijonegoro SragenDocument24 pagesKomplikasi Dalam Kehamilan: Dr. Dian Ika Putri Syafaruddin, Spog Smf. Obgyn Rsud Soehadi Prijonegoro SragenAldha S PutriiNo ratings yet
- QXR TB User GuideDocument12 pagesQXR TB User GuideBilly Omar Muñoz PeinadoNo ratings yet
- Hilary Di Santo Case NotesDocument2 pagesHilary Di Santo Case NotesNishu khobraNo ratings yet
- 2015 Neonatal AnesthesiaDocument464 pages2015 Neonatal AnesthesiajulianalaiscNo ratings yet
- Urinary CatheterizationDocument6 pagesUrinary CatheterizationLorenn AdarnaNo ratings yet
- Biotechnology Scientist or Lab Administrator or Assistant ProfesDocument7 pagesBiotechnology Scientist or Lab Administrator or Assistant Profesapi-79122341No ratings yet
- Overview of Nursing TheoriesDocument60 pagesOverview of Nursing TheoriestokzzNo ratings yet
- Medicine: Congenital Chloride Losing DiarrheaDocument9 pagesMedicine: Congenital Chloride Losing DiarrheaGabriela PopescuNo ratings yet
- Goldburg2019 PDFDocument43 pagesGoldburg2019 PDFsandeep lal vNo ratings yet
- Hypertension in PregnancyDocument31 pagesHypertension in PregnancyradhabobbyNo ratings yet
- Oropharyngeal and Nasopharyngeal Suctioning (Rationale)Document3 pagesOropharyngeal and Nasopharyngeal Suctioning (Rationale)Jemina Rafanan Racadio100% (2)
- Myusdoctor 150414122940 Conversion Gate01Document15 pagesMyusdoctor 150414122940 Conversion Gate01shipletNo ratings yet
- TeratologyDocument36 pagesTeratologySafera RezaNo ratings yet
- Literature Review: The Effect of Pronation Position On Hemodynamic Change in Premature Baby With RdsDocument9 pagesLiterature Review: The Effect of Pronation Position On Hemodynamic Change in Premature Baby With RdsIzmiatunNo ratings yet
- Oet Sample LetterDocument1 pageOet Sample LetterKhansa Rubab100% (1)
- Activity On Understanding VulnerabilityDocument3 pagesActivity On Understanding VulnerabilityLeila EnolpeNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)