You might also like
- Cyto B 10011Document5 pagesCyto B 10011Upgraders of the worldNo ratings yet
- Cytometry Part B Clinical - 2018 - Garcia Prat - Extended Immunophenotyping Reference Values in A Healthy PediatricDocument11 pagesCytometry Part B Clinical - 2018 - Garcia Prat - Extended Immunophenotyping Reference Values in A Healthy PediatricSabina-Gabriela MihaiNo ratings yet
- CBM Final PDFDocument7 pagesCBM Final PDFSamah Abd ElhamidNo ratings yet
- Utility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisDocument6 pagesUtility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisPablo VélezNo ratings yet
- Plasma Viral Load and CD4 Lymphocytes As Prognostic Markers of HIV-1 InfectionDocument9 pagesPlasma Viral Load and CD4 Lymphocytes As Prognostic Markers of HIV-1 InfectionStefania CristinaNo ratings yet
- Paediatric Reference Values For The Peripheral T Cell CompartmentDocument9 pagesPaediatric Reference Values For The Peripheral T Cell CompartmentSubhajitHajraNo ratings yet
- Abseso Hpeatico IncidenciaDocument8 pagesAbseso Hpeatico IncidenciaGabriela Cervantes MoralesNo ratings yet
- Lymphocyte Subset Analysis in Children with Frequent Upper Respiratory InfectionsDocument4 pagesLymphocyte Subset Analysis in Children with Frequent Upper Respiratory InfectionsjulianasanjayaNo ratings yet
- Immunology Letters: SciencedirectDocument6 pagesImmunology Letters: SciencedirectLaila Kurnia PramonoNo ratings yet
- Flowcytometric Assessment of Activated Cytotoxic T Cells in Rapid Diagnosis of Hemophagocytic Lymphohistiocytosis in Pediatric PatientsDocument1 pageFlowcytometric Assessment of Activated Cytotoxic T Cells in Rapid Diagnosis of Hemophagocytic Lymphohistiocytosis in Pediatric Patientsgocelij948No ratings yet
- Artigo 30Document7 pagesArtigo 30raudneimNo ratings yet
- Hta Ecv Lash M1 L1 RB1Document5 pagesHta Ecv Lash M1 L1 RB1Erick Méndez RodríguezNo ratings yet
- Idiopathic CD4 Lymphocytopenia: Natural History and Prognostic FactorsDocument9 pagesIdiopathic CD4 Lymphocytopenia: Natural History and Prognostic FactorsBagus PrawiroNo ratings yet
- Elevated Rates of Intracerebral Hemorrhage in Individuals From A US Clinical Care HIV CohortDocument7 pagesElevated Rates of Intracerebral Hemorrhage in Individuals From A US Clinical Care HIV CohortNani OktaviaNo ratings yet
- Research Paper On Hepatitis C PDFDocument6 pagesResearch Paper On Hepatitis C PDFfvf4r6xq100% (1)
- Original ArticleDocument6 pagesOriginal ArticlesarahhfitrianiNo ratings yet
- 14 2019 流式诊断陷阱Document15 pages14 2019 流式诊断陷阱huangzz1016No ratings yet
- Flow Cytometric Characterization of CD7+ Cell Subsets in Normal Bone Marrow for Diagnosis and Follow-Up of T-ALLDocument10 pagesFlow Cytometric Characterization of CD7+ Cell Subsets in Normal Bone Marrow for Diagnosis and Follow-Up of T-ALLKarla Novoa PérezNo ratings yet
- Predictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationDocument6 pagesPredictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationMuhammad Hafidzul HairulNo ratings yet
- ID48Document11 pagesID48AquarelinhasNo ratings yet
- Emergencias-2012 24 5 348-356 EngDocument9 pagesEmergencias-2012 24 5 348-356 EngJarvis WheelerNo ratings yet
- 2019 Article 4204Document9 pages2019 Article 4204Asep RiswandiNo ratings yet
- CD4CD8 Lymphocyte Counts in Healthy HIV-positive IDocument13 pagesCD4CD8 Lymphocyte Counts in Healthy HIV-positive ILaila Kurnia PramonoNo ratings yet
- Characterization of Immunophenotypic Aberrancies in Adult and Childhood Acute Lymphoblastic Leukemia Lessons From Regional VariationDocument7 pagesCharacterization of Immunophenotypic Aberrancies in Adult and Childhood Acute Lymphoblastic Leukemia Lessons From Regional VariationAzucena BCNo ratings yet
- AIJPMS - Volume 3 - Issue 1 - Pages 78-85Document8 pagesAIJPMS - Volume 3 - Issue 1 - Pages 78-85Eman MahmoudNo ratings yet
- Kanker TumorDocument11 pagesKanker TumorRENTI NOVITANo ratings yet
- Association Between Mitochondrial DNA Content in Leukocytes and Colorectal Cancer RiskDocument8 pagesAssociation Between Mitochondrial DNA Content in Leukocytes and Colorectal Cancer RiskMauro Porcel de PeraltaNo ratings yet
- Arneth 2015 Early Activation of CD and CD T LymDocument5 pagesArneth 2015 Early Activation of CD and CD T LymCarla Pabón FloresNo ratings yet
- The Pathophysiology of Pure Red Cell Aplasia: Implications For TherapyDocument9 pagesThe Pathophysiology of Pure Red Cell Aplasia: Implications For TherapyPhương NhungNo ratings yet
- The Natural History of Hepatitis C Virus Infection: Host, Viral, and Environmental FactorsDocument0 pagesThe Natural History of Hepatitis C Virus Infection: Host, Viral, and Environmental FactorsAnis Ur RahmanNo ratings yet
- 1307-Article Text-3852-1-10-20170616Document6 pages1307-Article Text-3852-1-10-20170616Dalila BackupNo ratings yet
- Total Cholesterol and All-Cause Mortality by Sex and Age: A Prospective Cohort Study Among 12.8 Million AdultsDocument10 pagesTotal Cholesterol and All-Cause Mortality by Sex and Age: A Prospective Cohort Study Among 12.8 Million AdultsNiklaus ItenNo ratings yet
- HCV in MexicoDocument8 pagesHCV in MexicoErwin Chiquete, MD, PhDNo ratings yet
- Isrn Oncology2012-652682Document7 pagesIsrn Oncology2012-652682Igoh Est Part IINo ratings yet
- Research Paper On Blood GroupsDocument4 pagesResearch Paper On Blood Groupshumin1byjig2100% (1)
- Outcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofDocument9 pagesOutcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofFrankenstein MelancholyNo ratings yet
- Cancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T CellDocument10 pagesCancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T Cell2512505993No ratings yet
- Comparison of Neutrophil CD64 Expression, Manual Myeloid Immaturity Counts, and Automated Hematology Analyzer Fla...Document12 pagesComparison of Neutrophil CD64 Expression, Manual Myeloid Immaturity Counts, and Automated Hematology Analyzer Fla...Reyhan IsmNo ratings yet
- Cardiovascular Risk Factors Among Young AdultsDocument8 pagesCardiovascular Risk Factors Among Young AdultsJuan Alejandro Bastidas VejarNo ratings yet
- Normal Range of CD4 Cell Counts and Temporal Changes in Two HIV-Negative Malawian PopulationsDocument6 pagesNormal Range of CD4 Cell Counts and Temporal Changes in Two HIV-Negative Malawian PopulationsTin Aung KyiNo ratings yet
- ILN Biomarker 2016Document6 pagesILN Biomarker 2016AlienNo ratings yet
- CCDT Cancer ProteomicsDocument37 pagesCCDT Cancer ProteomicsRakesh InnovationsAnd SolutionsInstituteNo ratings yet
- Association Between Benign Thyroid Disease and Breast Cancer: A Single Center ExperienceDocument8 pagesAssociation Between Benign Thyroid Disease and Breast Cancer: A Single Center ExperiencelolaNo ratings yet
- Biol Blood Marrow Transplant 2020 26 10 1828-32Document5 pagesBiol Blood Marrow Transplant 2020 26 10 1828-32Fernando SousaNo ratings yet
- s12981 018 0200 4Document9 pagess12981 018 0200 4nazilia khaerunnisaNo ratings yet
- PCT FeverDocument6 pagesPCT FeverAndi BintangNo ratings yet
- Research: ArticleDocument4 pagesResearch: ArticleMuthu KumarNo ratings yet
- Diagnostic Criteria For Tuberculous MeningitisDocument5 pagesDiagnostic Criteria For Tuberculous MeningitisbidisNo ratings yet
- Tumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerDocument9 pagesTumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerWilliamRayCassidyNo ratings yet
- Carey 2005 CD4 Quantitation HIV + Child Antiretroviral TXDocument4 pagesCarey 2005 CD4 Quantitation HIV + Child Antiretroviral TXMaya RustamNo ratings yet
- Circulating Serum Markers and QRS Scar Score in Chagas Cardiomyopathy 2015Document6 pagesCirculating Serum Markers and QRS Scar Score in Chagas Cardiomyopathy 2015Laura montillaNo ratings yet
- Investigating Multi-Cancer Biomarkers and Their Cross-Predictability in The Expression Profiles of Multiple Cancer TypesDocument23 pagesInvestigating Multi-Cancer Biomarkers and Their Cross-Predictability in The Expression Profiles of Multiple Cancer TypesXavierNo ratings yet
- Jurnal Kunci NMLRDocument6 pagesJurnal Kunci NMLRDwika AudiyanandaNo ratings yet
- To Study Haematological Profile of Enteric Fever Patients.: International Journal of Current Research in Medical SciencesDocument6 pagesTo Study Haematological Profile of Enteric Fever Patients.: International Journal of Current Research in Medical SciencesAnonymous hF9HwHVuqNo ratings yet
- Diagnostic Microbiology and Infectious DiseaseDocument5 pagesDiagnostic Microbiology and Infectious DiseasefranciscoreynaNo ratings yet
- Artigo para DiscussãoDocument8 pagesArtigo para Discussãomarcos.vinicius.c2151No ratings yet
- Can PCT help differentiate bacterial infection from inflammationDocument5 pagesCan PCT help differentiate bacterial infection from inflammationAndi BintangNo ratings yet
- Early Atherosclerosis in Rheumatoid Arthritis: A Case Control StudyDocument5 pagesEarly Atherosclerosis in Rheumatoid Arthritis: A Case Control StudychandanNo ratings yet
- Img#Document5 pagesImg#AngelNo ratings yet
- Sample Questions 2019Document6 pagesSample Questions 2019أحہمہد بہنہ قہمہوNo ratings yet
- MD/MPH Capstone TimelineDocument3 pagesMD/MPH Capstone Timelineأحہمہد بہنہ قہمہوNo ratings yet
- Rubric Ms PHD For SP 2020 and Beyond PDFDocument5 pagesRubric Ms PHD For SP 2020 and Beyond PDFأحہمہد بہنہ قہمہوNo ratings yet
- Comprehensive Medicinal Chemistry: Corwin HanschDocument6 pagesComprehensive Medicinal Chemistry: Corwin Hanschأحہمہد بہنہ قہمہوNo ratings yet
- University of Miami Miller School of Medicine Department of Public Health Sciences Resiliency Scholarship ProgramDocument2 pagesUniversity of Miami Miller School of Medicine Department of Public Health Sciences Resiliency Scholarship Programأحہمہد بہنہ قہمہوNo ratings yet
- Evolution and Pathogenesis Of: Lessons Learned From Genotyping and Comparative GenomicsDocument15 pagesEvolution and Pathogenesis Of: Lessons Learned From Genotyping and Comparative Genomicsأحہمہد بہنہ قہمہوNo ratings yet
- NSAIDs Lecture 2 Mechanism of Action and ClassificationDocument12 pagesNSAIDs Lecture 2 Mechanism of Action and Classificationأحہمہد بہنہ قہمہوNo ratings yet
- Ni Hms 759622Document21 pagesNi Hms 759622أحہمہد بہنہ قہمہوNo ratings yet
- ISO 13485 Version 2016 Requirements NotesDocument24 pagesISO 13485 Version 2016 Requirements Notesda_reaper_dasNo ratings yet
- The Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsDocument22 pagesThe Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsBabar MairajNo ratings yet
- Cooler Ok El8sDocument11 pagesCooler Ok El8sIBRAHIM ALMANLANo ratings yet
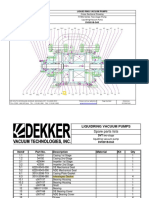
- Bomba de Vacio Part ListDocument2 pagesBomba de Vacio Part ListNayeli Zarate MNo ratings yet
- Semiconductor Optical AmplifierDocument40 pagesSemiconductor Optical AmplifierVikas ThakurNo ratings yet
- Pag-IBIG Employer Enrollment FormDocument1 pagePag-IBIG Employer Enrollment FormDarlyn Etang100% (1)
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet
- WMS INFINEON PROJECT TOWER (11Kv VCB INSTALLATION) - REV-1Document5 pagesWMS INFINEON PROJECT TOWER (11Kv VCB INSTALLATION) - REV-1tana100% (1)
- MPX English Final Version VOLUME 3Document878 pagesMPX English Final Version VOLUME 3Adrian MacayaNo ratings yet
- Critical Buckling Load of Pile in Liquefied SoilDocument8 pagesCritical Buckling Load of Pile in Liquefied SoilKefas JanuarNo ratings yet
- DownloadDocument2 pagesDownloadAmit KumarNo ratings yet
- String inverter comparisonDocument4 pagesString inverter comparisonRakesh HateyNo ratings yet
- What is phonicsDocument244 pagesWhat is phonicsNelly FernandezNo ratings yet
- Lab Practice # 01 An Introduction To MatlabDocument10 pagesLab Practice # 01 An Introduction To MatlabGhulam Abbas LashariNo ratings yet
- 2017 Expert Packet Workshop V3 + ExerciseDocument268 pages2017 Expert Packet Workshop V3 + ExerciseJeya ChandranNo ratings yet
- Foundations On Expansive Soils: 3.1. BackgroundDocument31 pagesFoundations On Expansive Soils: 3.1. BackgroundbiniNo ratings yet
- Bachelor of Arts (Psychology HR Management) Y3 V2Document1 pageBachelor of Arts (Psychology HR Management) Y3 V2Kenny sylvainNo ratings yet
- Chapter 22A - Sound WavesDocument24 pagesChapter 22A - Sound Wavesqwivy.comNo ratings yet
- Were in The City of Palu in Central Sulawesi, IndonesiaDocument5 pagesWere in The City of Palu in Central Sulawesi, IndonesiaTú AnhNo ratings yet
- But Virgil Was Not There": The Lasting Impact of Dante's Homosocial HellDocument7 pagesBut Virgil Was Not There": The Lasting Impact of Dante's Homosocial HellЮлия ЧебанNo ratings yet
- Bee WareDocument49 pagesBee WareJayNo ratings yet
- Narrative Report of Landfill VisitDocument3 pagesNarrative Report of Landfill VisitNestor Jan Kenneth P BorromeoNo ratings yet
- 02.casebook - BLDG Repairs & Maint - Chapter 1 - 2011 (Water Seepage)Document13 pages02.casebook - BLDG Repairs & Maint - Chapter 1 - 2011 (Water Seepage)Hang kong TseNo ratings yet
- HORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Document1 pageHORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Inna PotesNo ratings yet
- Rotorvane Tea OrthodoxDocument9 pagesRotorvane Tea OrthodoxyurinaNo ratings yet
- Anxiety, Depression and Self-Esteem in Children With Well-Controlled AsthmaDocument6 pagesAnxiety, Depression and Self-Esteem in Children With Well-Controlled AsthmaAbdallah H. KamelNo ratings yet
- Cultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinDocument54 pagesCultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinyhoulhandhariNo ratings yet
- Omega: Mahdi Alinaghian, Nadia ShokouhiDocument15 pagesOmega: Mahdi Alinaghian, Nadia ShokouhiMohcine ES-SADQINo ratings yet
- Goethe Zertifikat b1 HorenDocument2 pagesGoethe Zertifikat b1 HorenLevent75% (4)
- Sop For FatDocument6 pagesSop For Fatahmed ismailNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Tales from Both Sides of the Brain: A Life in NeuroscienceFrom EverandTales from Both Sides of the Brain: A Life in NeuroscienceRating: 3 out of 5 stars3/5 (18)
- Fast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperFrom EverandFast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperRating: 4.5 out of 5 stars4.5/5 (15)
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionFrom EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionRating: 4 out of 5 stars4/5 (811)
- The Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorFrom EverandThe Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorNo ratings yet
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessFrom Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessRating: 4 out of 5 stars4/5 (33)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- All That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesFrom EverandAll That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesRating: 4.5 out of 5 stars4.5/5 (397)
- Who's in Charge?: Free Will and the Science of the BrainFrom EverandWho's in Charge?: Free Will and the Science of the BrainRating: 4 out of 5 stars4/5 (65)
- Undeniable: How Biology Confirms Our Intuition That Life Is DesignedFrom EverandUndeniable: How Biology Confirms Our Intuition That Life Is DesignedRating: 4 out of 5 stars4/5 (11)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsFrom EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsRating: 4.5 out of 5 stars4.5/5 (4)
- Good Without God: What a Billion Nonreligious People Do BelieveFrom EverandGood Without God: What a Billion Nonreligious People Do BelieveRating: 4 out of 5 stars4/5 (66)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceFrom EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceRating: 4.5 out of 5 stars4.5/5 (515)
- The Consciousness Instinct: Unraveling the Mystery of How the Brain Makes the MindFrom EverandThe Consciousness Instinct: Unraveling the Mystery of How the Brain Makes the MindRating: 4.5 out of 5 stars4.5/5 (93)
- Inside of a Dog: What Dogs See, Smell, and KnowFrom EverandInside of a Dog: What Dogs See, Smell, and KnowRating: 4 out of 5 stars4/5 (390)
- Wayfinding: The Science and Mystery of How Humans Navigate the WorldFrom EverandWayfinding: The Science and Mystery of How Humans Navigate the WorldRating: 4.5 out of 5 stars4.5/5 (18)
- This Is Your Brain On Parasites: How Tiny Creatures Manipulate Our Behavior and Shape SocietyFrom EverandThis Is Your Brain On Parasites: How Tiny Creatures Manipulate Our Behavior and Shape SocietyRating: 3.5 out of 5 stars3.5/5 (31)
- Why We Sleep: Unlocking the Power of Sleep and DreamsFrom EverandWhy We Sleep: Unlocking the Power of Sleep and DreamsRating: 4.5 out of 5 stars4.5/5 (2083)
- Crypt: Life, Death and Disease in the Middle Ages and BeyondFrom EverandCrypt: Life, Death and Disease in the Middle Ages and BeyondRating: 4 out of 5 stars4/5 (3)
- A Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouFrom EverandA Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouRating: 4.5 out of 5 stars4.5/5 (62)
- The Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsFrom EverandThe Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsNo ratings yet
- The Invention of Tomorrow: A Natural History of ForesightFrom EverandThe Invention of Tomorrow: A Natural History of ForesightRating: 4.5 out of 5 stars4.5/5 (5)